

This is a preprint.
A Dual-Center Cohort Study on The Association Between Early Deep Sedation and Clinical Outcomes in Mechanically Ventilated Patients During the COVID-19 Pandemic: the COVID-SED Study
- PMID: 35262073
- PMCID: PMC8902881
- DOI: 10.21203/rs.3.rs-1389892/v1
A Dual-Center Cohort Study on The Association Between Early Deep Sedation and Clinical Outcomes in Mechanically Ventilated Patients During the COVID-19 Pandemic: the COVID-SED Study
Update in
-
A dual-center cohort study on the association between early deep sedation and clinical outcomes in mechanically ventilated patients during the COVID-19 pandemic: The COVID-SED study.Crit Care. 2022 Jun 15;26(1):179. doi: 10.1186/s13054-022-04042-9. Crit Care. 2022. PMID: 35705989 Free PMC article.
Abstract
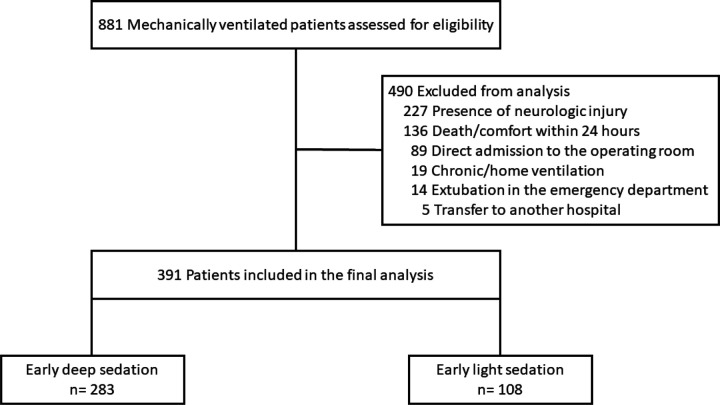
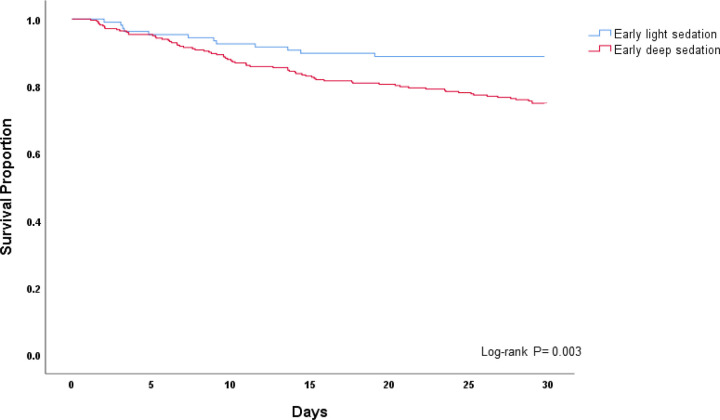
Background : Mechanically ventilated patients have experienced greater periods of prolonged deep sedation during the coronavirus disease (COVID-19) pandemic. Multiple studies from the pre-COVID era demonstrate that early deep sedation is associated with worse outcome. Despite this, there is a lack of data on sedation depth and its impact on outcome for mechanically ventilated patients during the COVID-19 pandemic. We sought to characterize the emergency department (ED) and intensive care unit (ICU) sedation practices during the COVID-19 pandemic, and to determine if early deep sedation was associated with worse clinical outcomes. Study Design and Methods : Dual-center, retrospective cohort study conducted over six months (March - August, 2020), involving consecutive, mechanically ventilated adults. All sedation-related data during the first 48 hours were collected. Deep sedation was defined as Richmond Agitation-Sedation Scale of -3 to -5 or Riker Sedation-Agitation Scale of 1 - 3. To examine impact of early sedation depth on hospital mortality (primary outcome) we used a multivariable logistic regression model. Secondary outcomes included ventilator-, ICU-, and hospital-free days. Results : 391 patients were studied, and 283 (72.4%) experienced early deep sedation. Deeply sedated patients received higher cumulative doses of fentanyl, propofol, midazolam, and ketamine when compared to light sedation. Deep sedation patients experienced fewer ventilator-, ICU-, and hospital-free days, and greater mortality (30.4% versus 11.1%) when compared to light sedation ( p < 0.01 for all). After adjusting for confounders, early deep sedation remained significantly associated with higher mortality (adjusted OR 3.44; 95% CI 1.65 - 7.17; p <0.01). These results were stable in the subgroup of patients with COVID-19. Conclusions : The management of sedation for mechanically ventilated patients in the ICU has changed during the COVID pandemic. Early deep sedation is common and independently associated with worse clinical outcomes. A protocol-driven approach to sedation, targeting light sedation as early as possible, should continue to remain the default approach. Clinical Trial Registration : Not applicable.
Conflict of interest statement
Competing Interests
All authors report no competing interests
Figures
Similar articles
-
A dual-center cohort study on the association between early deep sedation and clinical outcomes in mechanically ventilated patients during the COVID-19 pandemic: The COVID-SED study.Crit Care. 2022 Jun 15;26(1):179. doi: 10.1186/s13054-022-04042-9. Crit Care. 2022. PMID: 35705989 Free PMC article.
-
Analgosedation Practices and the Impact of Sedation Depth on Clinical Outcomes Among Patients Requiring Mechanical Ventilation in the ED: A Cohort Study.Chest. 2017 Nov;152(5):963-971. doi: 10.1016/j.chest.2017.05.041. Epub 2017 Jun 21. Chest. 2017. PMID: 28645462 Free PMC article.
-
The ED-SED Study: A Multicenter, Prospective Cohort Study of Practice Patterns and Clinical Outcomes Associated With Emergency Department SEDation for Mechanically Ventilated Patients.Crit Care Med. 2019 Nov;47(11):1539-1548. doi: 10.1097/CCM.0000000000003928. Crit Care Med. 2019. PMID: 31393323 Free PMC article.
-
Practice Patterns and Outcomes Associated With Early Sedation Depth in Mechanically Ventilated Patients: A Systematic Review and Meta-Analysis.Crit Care Med. 2018 Mar;46(3):471-479. doi: 10.1097/CCM.0000000000002885. Crit Care Med. 2018. PMID: 29227367 Free PMC article.
-
Managing sedation in the mechanically ventilated emergency department patient: a clinical review.J Am Coll Emerg Physicians Open. 2020 Apr 10;1(3):263-269. doi: 10.1002/emp2.12045. eCollection 2020 Jun. J Am Coll Emerg Physicians Open. 2020. PMID: 33000041 Free PMC article. Review.
References
-
- Morris PE, Goad A, Thompson C, Taylor K, Harry B, Passmore L, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Critical care medicine. 2008;36(8):2238–43. - PubMed
-
- Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. New England journal of medicine. 2006;355(26):2725–32. - PubMed
-
- Network ARDS, Wheeler A, Bernard G, Thompson B, Hayden D, DeBoisblanc B. Comparison of two fluid-management strategies in acute lung injury. N Engl j Med. 2006;354(24):2564–75. - PubMed
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342(18):1301–8. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
