

Ventricular Synchrony in Para-Hisian Cardiac Pacing as an Alternative for Physiological Cardiac Activation (Indirect Recruitment of the His Bundle?)
- PMID: 35262586
- PMCID: PMC8856677
- DOI: 10.36660/abc.20201233
Ventricular Synchrony in Para-Hisian Cardiac Pacing as an Alternative for Physiological Cardiac Activation (Indirect Recruitment of the His Bundle?)
Abstract
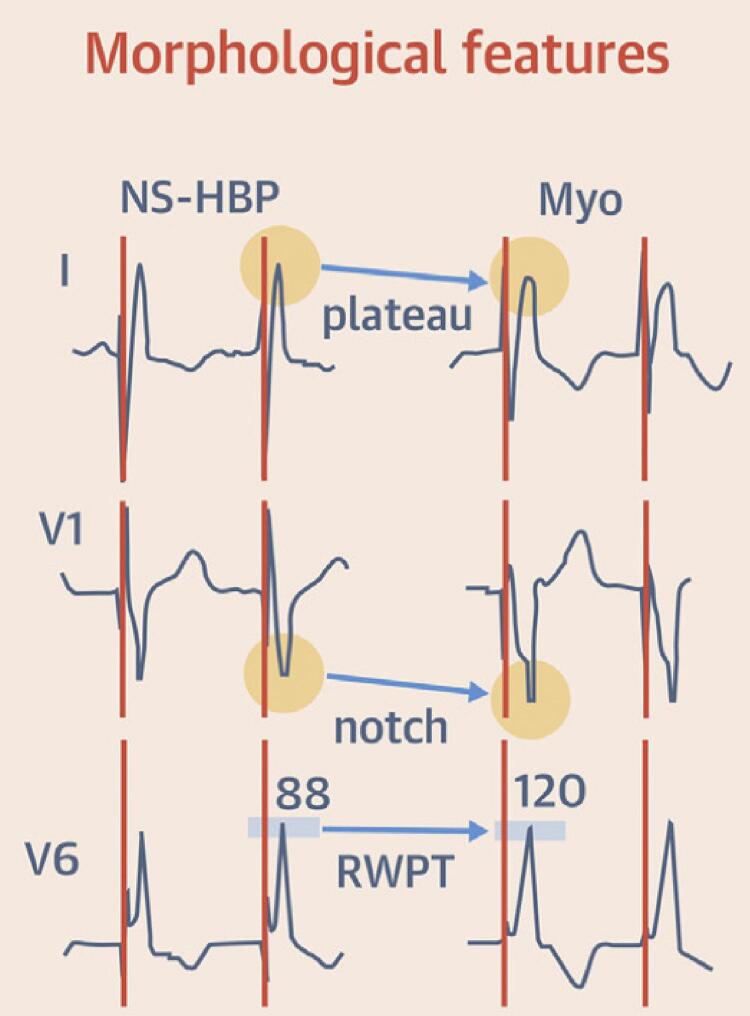
Background: Artificial cardiac pacing by direct or indirect His bundle capture results in synchronous ventricular contraction (physiological pacing).
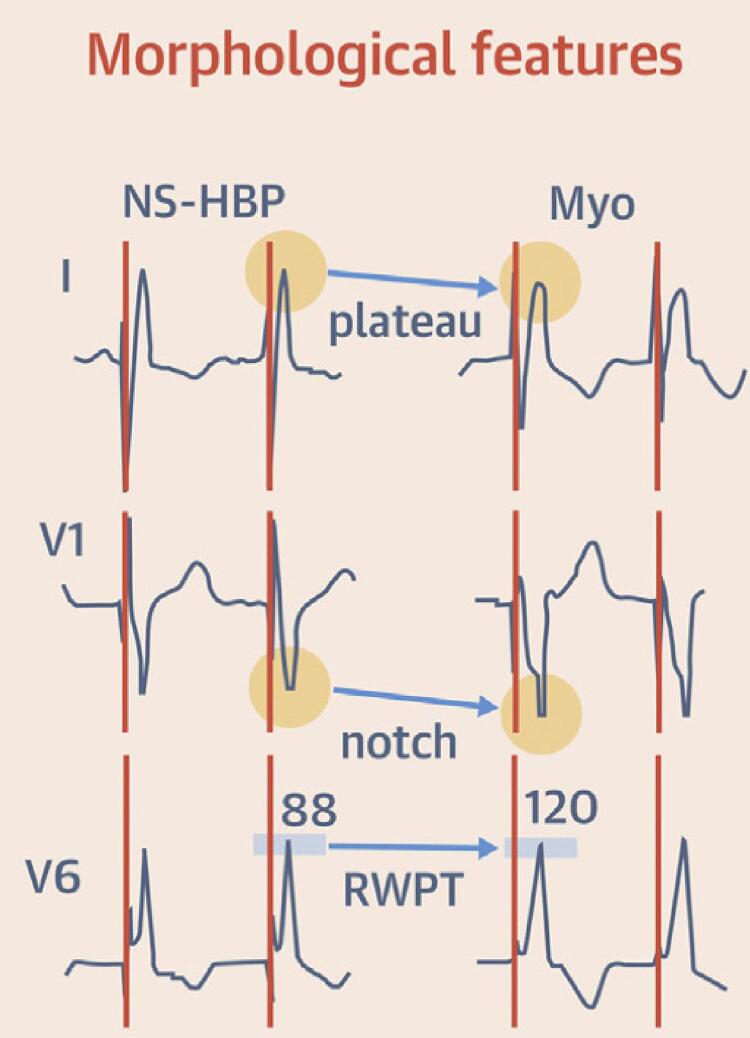
Objectives: To compare cardiac synchronization, technical characteristics, and electronic parameters between two techniques of indirect His-bundle pacing: non-selective (NS-HBP) vs para-Hisian pacing (PHP).
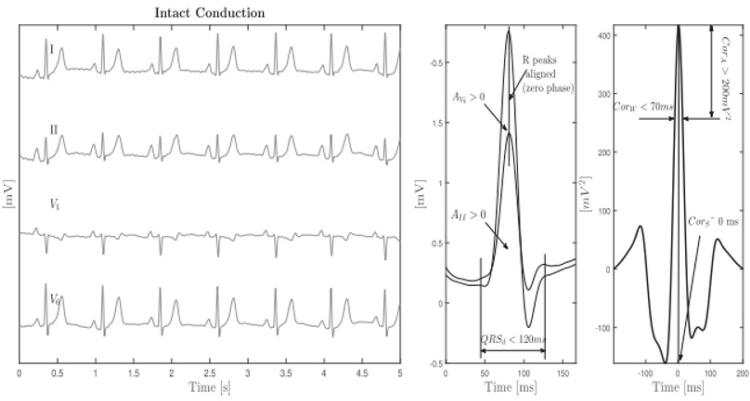
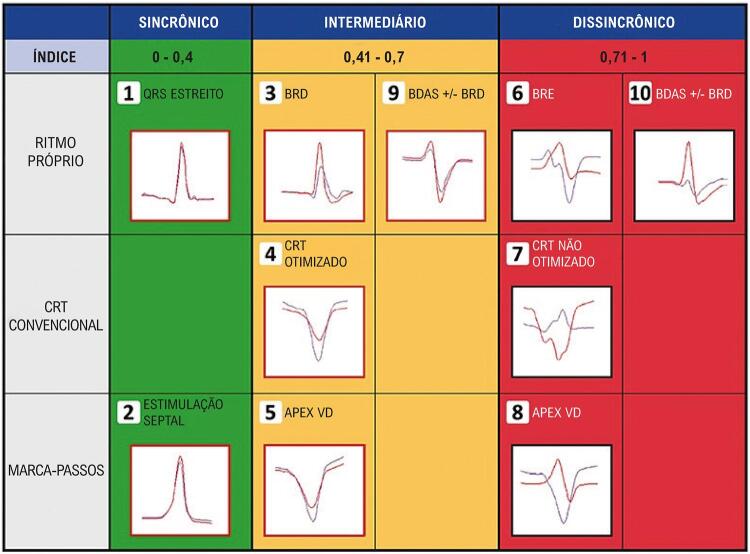
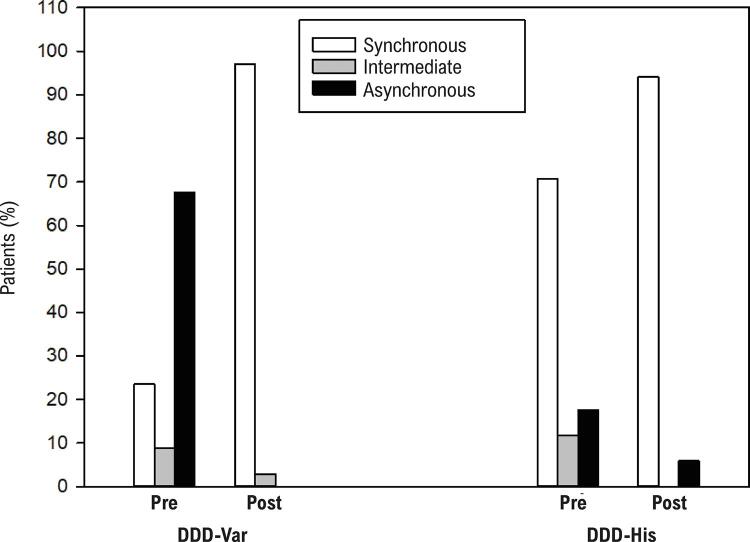
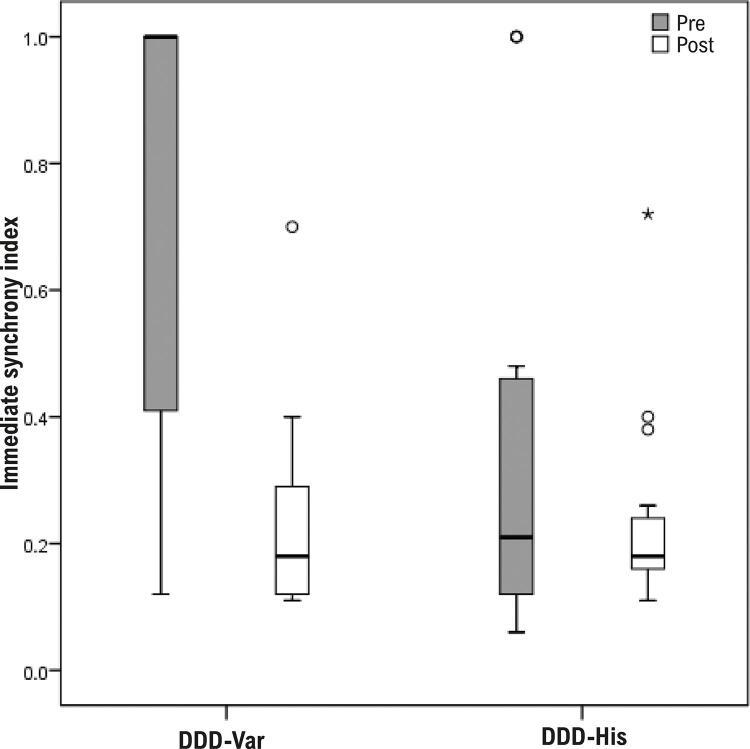
Methods: The experimental intervention (between November 2019 and April 2020) consisted of implanting a DDD pacemaker in patients who had left ventricular ejection fraction (LVEF) > 35%. The resulting cardiac synchronization was compared using an electrocardiographic algorithm that analyzed QRS variation and the technical characteristics of non-selective Hisian pacing (DDD-His) and para-Hisian pacing (DDD-Var).
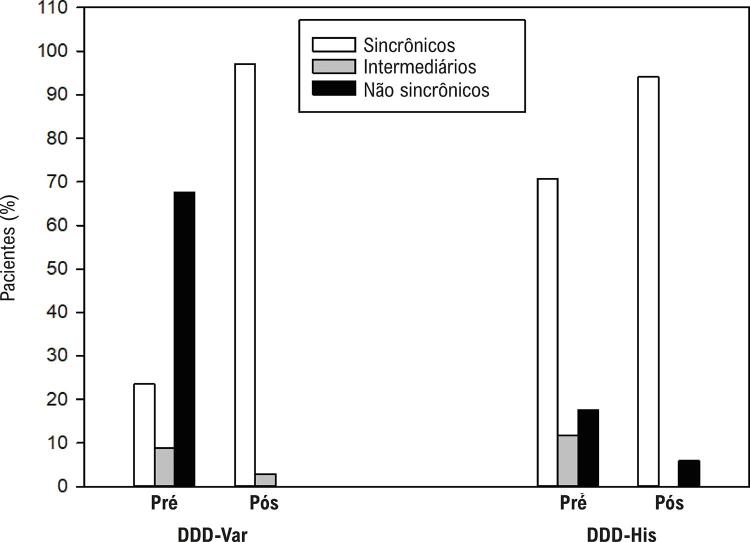
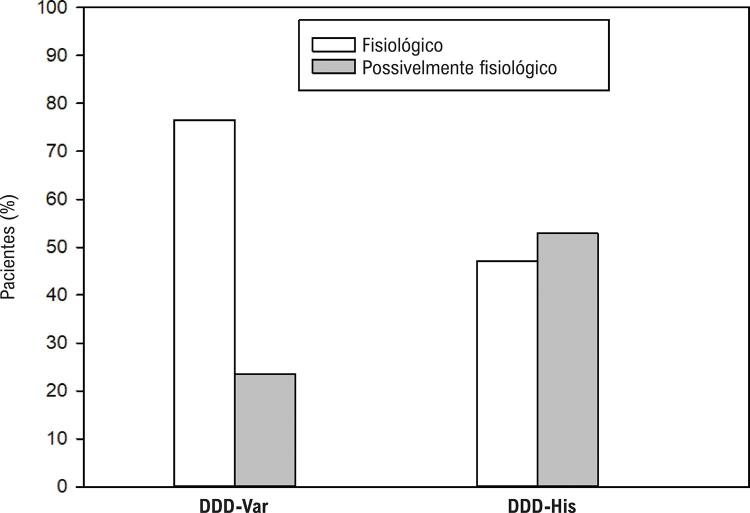
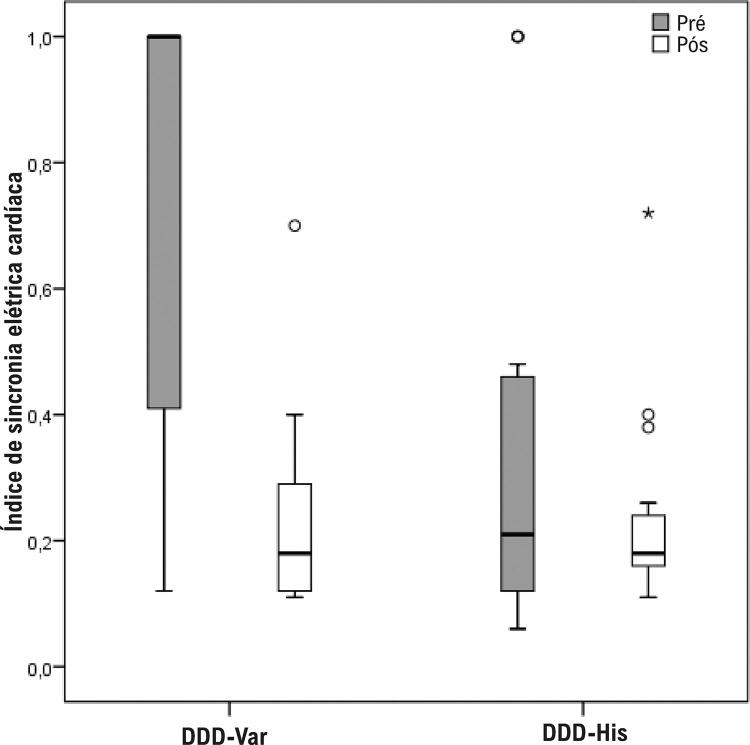
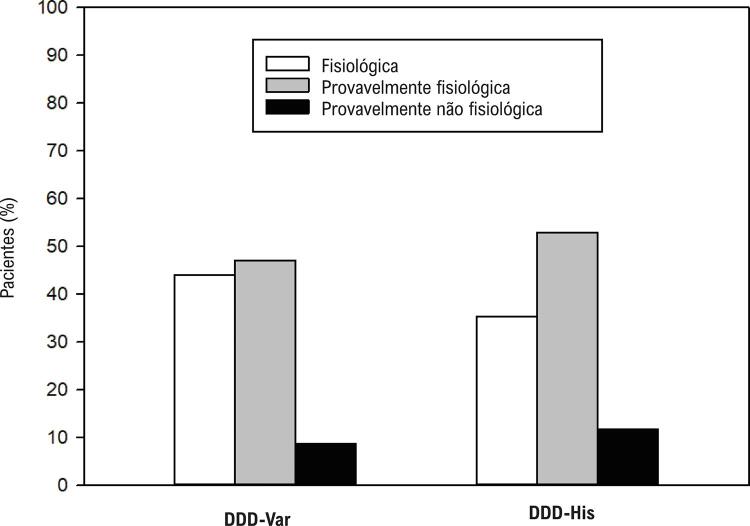
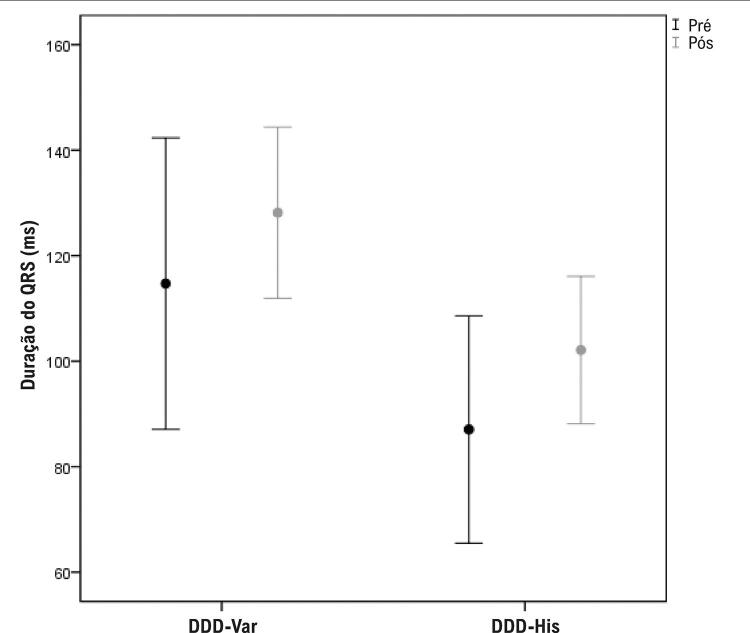
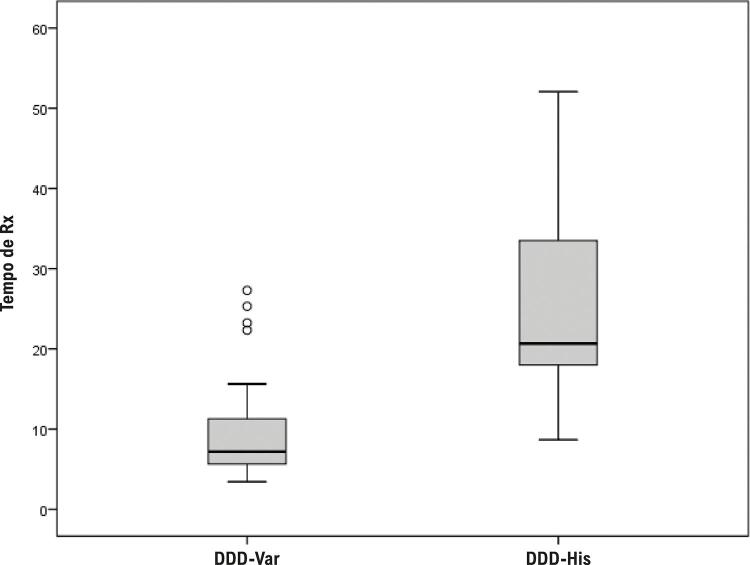
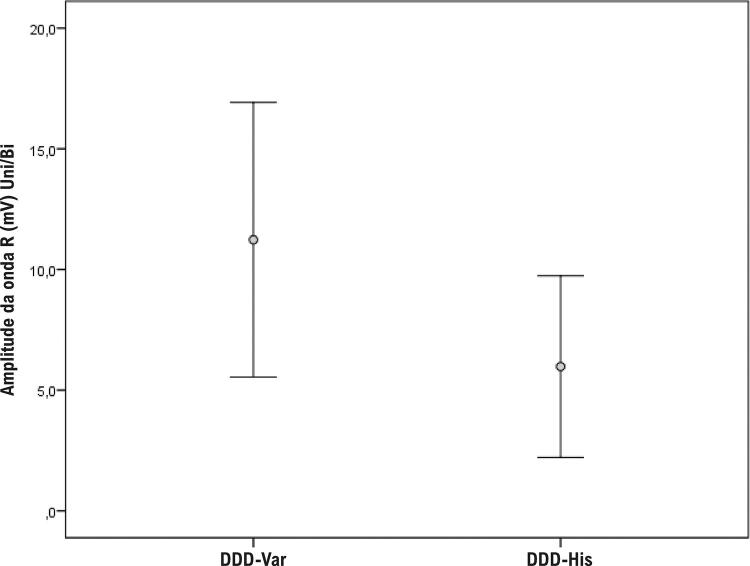
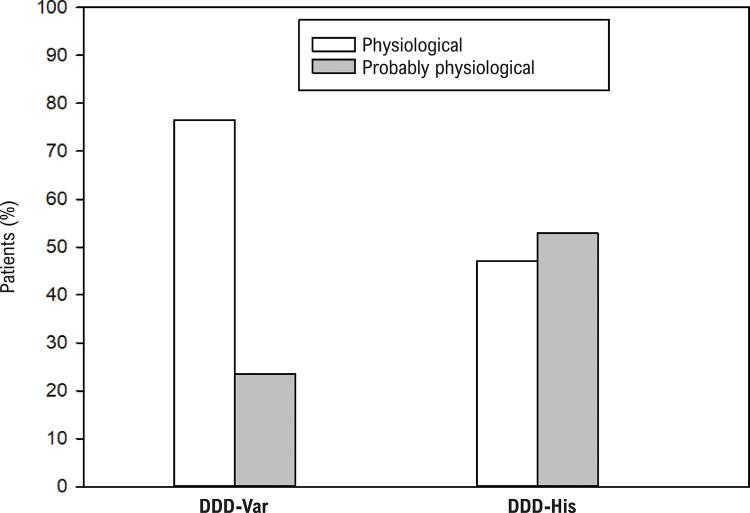
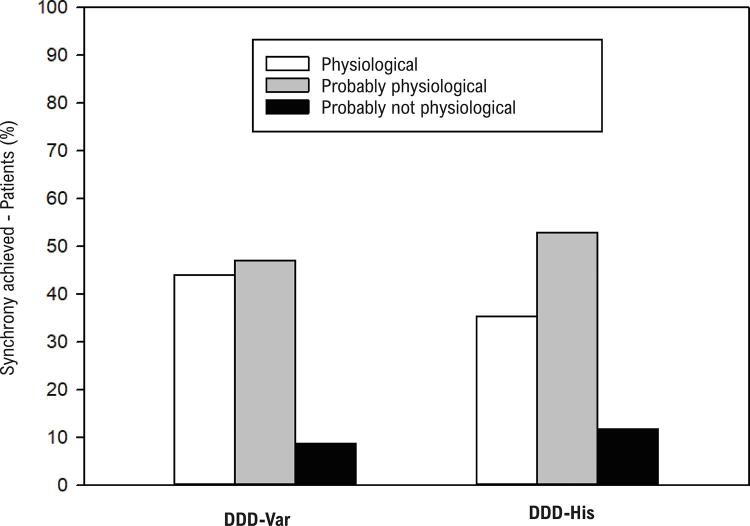
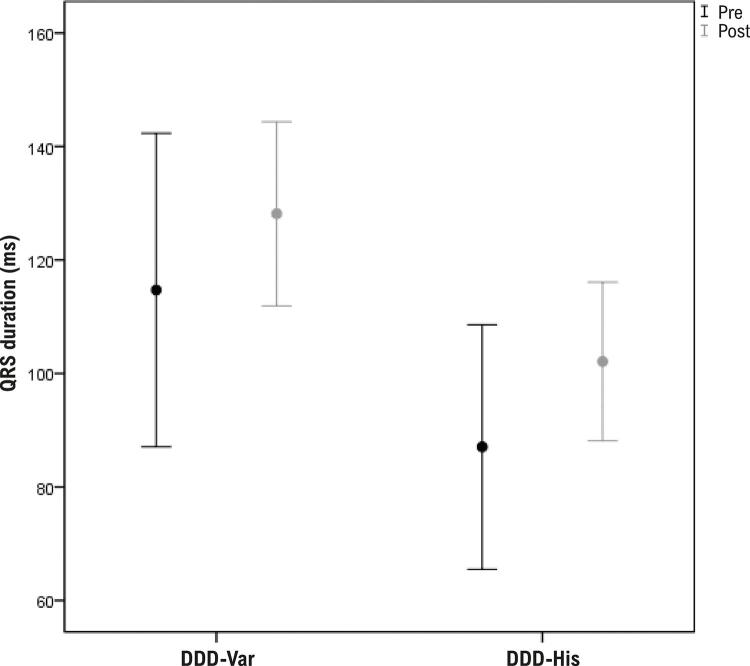
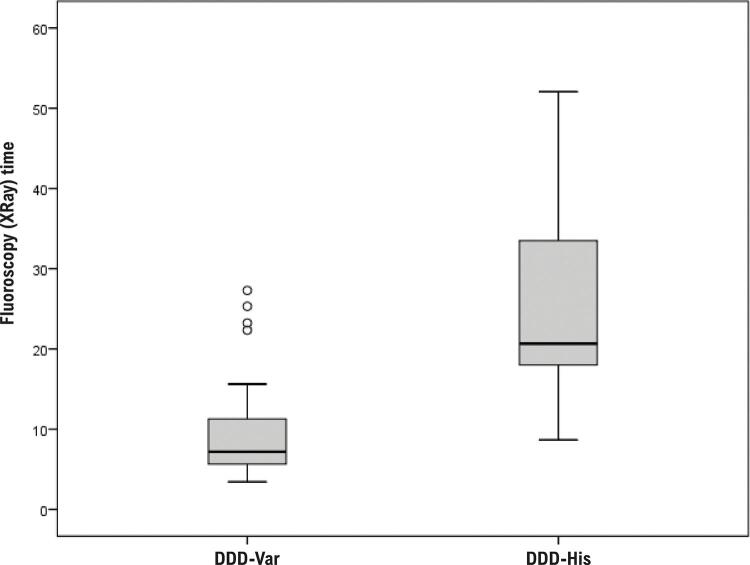
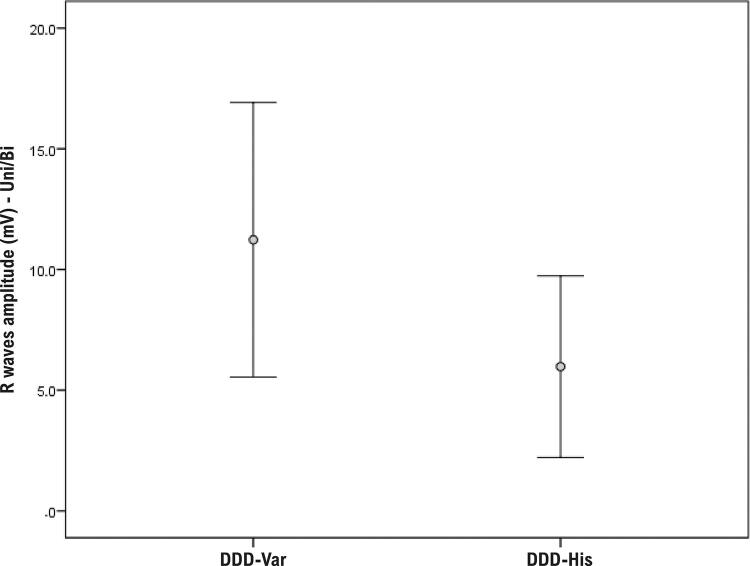
Results: Of 51 total patients (men: 28), 66.7% (34) were allocated to the DDD-Var group and 33.3% (17) to the DDD-His group. The mean ages in each group were 74 and 79 years, respectively. In the DDD-Var group, QRS variation (ventricular synchrony) improved after implantation (p < 0.001). In post-implantation ECG, 91.2% of the DDD-Var group presented a physiological pacing pattern, which was similar to the DDD-His group (88.2%; p = 0.999). The paced QRS axis was also similar (physiological) for both groups. Intraoperative fluoroscopy time (XRay) during implantation was lower for the para-Hisian technique (median 7 min in the DDD-Var group vs 21 min in the DDD-His group, p < 0.001). The mean QRS duration increased in the DDD-Var group (114.7 ms pre-implantation vs 128.2 ms post-implantation, p = 0.044). The mean post-implantation R-wave amplitude was 11.2 mV in the DDD-Var group vs 6.0 mV in the DDD-His group, p = 0.001.
Conclusion: Para-Hisian pacing appears to indirectly recruit the His bundle, which would make this an effective and comparable strategy for physiological pacing, resulting in synchronous ventricular contraction similar to that of non-selective Hisian pacing.
Fundamento: A estimulação cardíaca artificial (ECA) por captura direta ou indireta do feixe de His resulta em contração ventricular sincrônica (ECA fisiológica).
Objetivos: Comparar sincronia cardíaca, características técnicas e resultados de parâmetros eletrônicos entre duas técnicas de ECA indireta do feixe de His: a não seletiva e a parahissiana.
Métodos: Intervenção experimental (novembro de 2019 a abril de 2020) com implante de marca-passo definitivo (MPd) DDD em pacientes com fração de ejeção ventricular esquerda > 35%. Foram comparadas a sincronia cardíaca resultante mediante algoritmo de análise eletrocardiográfica da variância espacial do QRS e as características técnicas associadas a cada método entre ECA hissiana não seletiva (DDD-His) e parahissiana (DDD-Var).
Resultados: De 51 pacientes (28 homens), 34 (66,7%) foram alocados no grupo DDD-Var e 17 (33,3%), no grupo DDD-His, com idade média de 74 e 79 anos, respectivamente. No grupo DDD-Var, a análise da variância espacial do QRS (índice de sincronia ventricular) mostrou melhora após o implante de MPd (p < 0,001). Ao ECG pós-implante, 91,2% dos pacientes do grupo DDD-Var mostraram padrão fisiológico de ECA, comprovando ativação similar à do DDD-His (88,2%; p = 0,999). O eixo do QRS estimulado também foi similar (fisiológico) para ambos os grupos. A mediana do tempo de fluoroscopia do implante foi de 7 minutos no grupo DDD-Var e de 21 minutos no DDD-His (p < 0,001), favorecendo a técnica parahissiana. A duração média do QRS aumentou nos pacientes do DDD-Var (114,7 ms pré-MPd e 128,2 ms pós-implante, p = 0,044). A detecção da onda R foi de 11,2 mV no grupo DDD-Var e de 6,0 mV no DDD-His (p = 0,001).
Conclusão: A ECA parahissiana comprova recrutamento indireto do feixe de His, mostrando-se uma estratégia eficaz e comparável à ECA fisiológica ao resultar em contração ventricular sincrônica similar à obtida por captura hissiana não seletiva.
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures


Comment in
-
Parahissian Cardiac Stimulation - New Alternative for More Physiological Stimulation of the Heart?Arq Bras Cardiol. 2022 Feb;118(2):503-504. doi: 10.36660/abc.20220016. Arq Bras Cardiol. 2022. PMID: 35262587 Free PMC article. English, Portuguese. No abstract available.
References
-
- Cho SW, Gwag HB, Hwang JK, Chun KJ, Park KM, On YK, et al. Clinical Features, Predictors, and Long-Term Prognosis of Pacing-Induced Cardiomyopathy. Eur J Heart Fail. 2019;21(5):643-51. doi: 10.1002/ejhf.1427. - PubMed
-
- Matusik PT. Adverse Clinical Outcomes Related to Right Ventricular Pacing. Eur Heart J. 2019;40(20):1586-88. doi: 10.1093/eurheartj/ehz279. - PubMed
-
- Ferrari ADL. Avaliação de Dessincronia Atrioventricular em Portadores de Marca-Passo Bicameral Devido a Doença do Nó Sinusal e Bloqueio Atrioventricular de Primeiro Grau [dissertation]. São Paulo: Universidade de São Paulo; 2017. doi: 10.11606/T.98.2017.tde-05102017-074636.
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
