

Spectrum of Nonkeratinocyte Skin Cancer Risk Among Solid Organ Transplant Recipients in the US
- PMID: 35262623
- PMCID: PMC8908231
- DOI: 10.1001/jamadermatol.2022.0036
Spectrum of Nonkeratinocyte Skin Cancer Risk Among Solid Organ Transplant Recipients in the US
Abstract
Importance: Nonkeratinocyte skin cancers are an important cause of morbidity and mortality for immunosuppressed solid organ transplant recipients (SOTRs), but the spectrum of disease and risk factor characteristics are unknown.
Objective: To characterize the spectrum of disease and risk factors for common and rare nonkeratinocyte skin cancers in SOTRs.
Design, setting, and participants: This population-based cohort study included 444 497 SOTRs who underwent a transplant in the US between January 1, 1987, and December 31, 2017, using linked data from the national transplant registry and 32 cancer registries. Data analysis was conducted from April 1, 2021, to September 30, 2021.
Main outcomes and measures: Standardized incidence ratios (SIRs) were used to assess risk relative to the general population, and Poisson regression was used to evaluate risk factors.
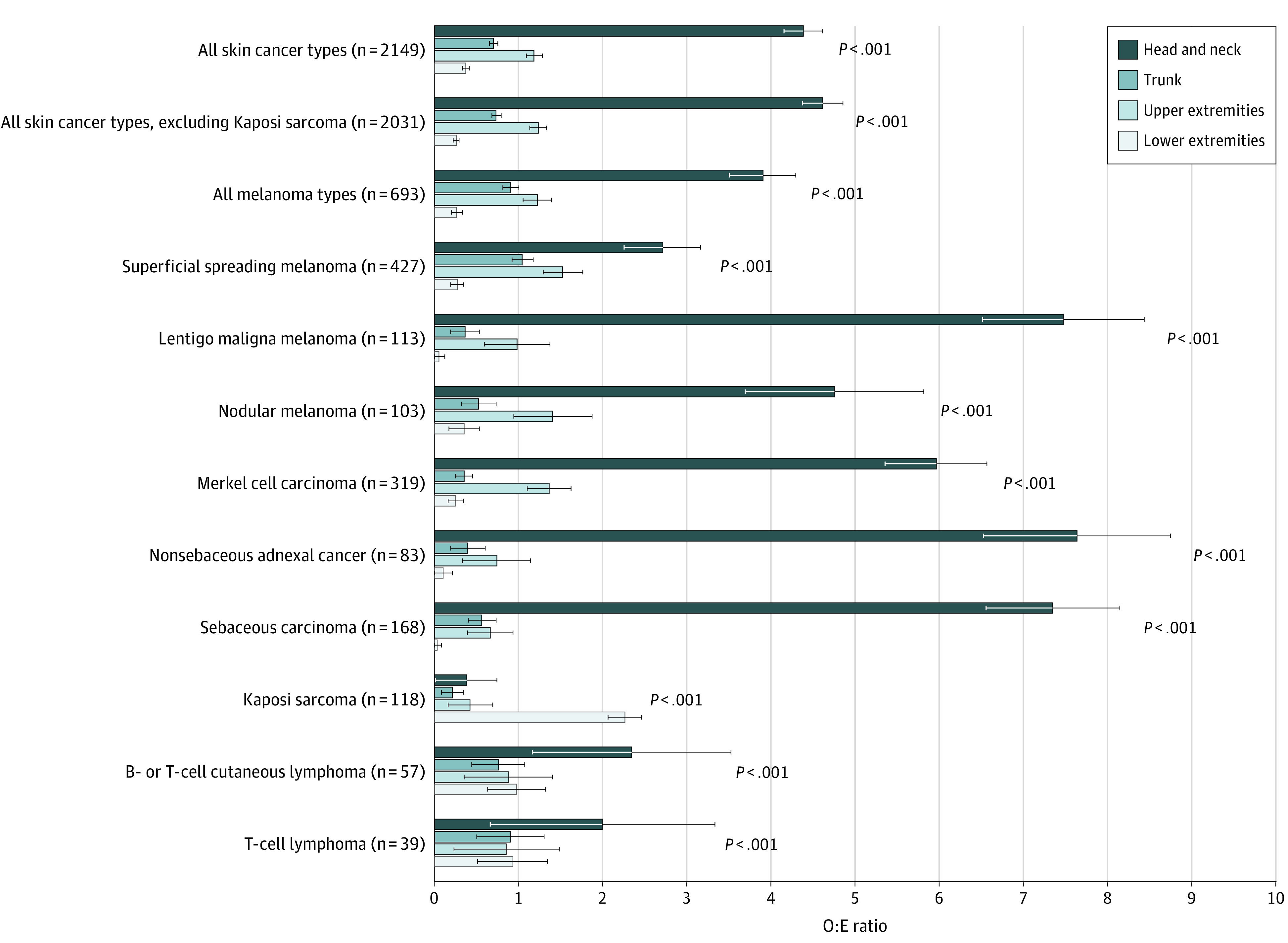
Results: A total of 2380 nonkeratinocyte skin cancers were identified among 444 497 SOTRs (median age at transplant, 50 years; range, 0-96 years; 274 276 [61.7%] male; 272 241 [61.2%] non-Hispanic White). Melanoma was the most common cancer (1471 [61.8%]), followed by Merkel cell carcinoma (334 [14.0%]), Kaposi sarcoma (186 [7.8%]), sebaceous carcinoma (170 [7.1%]), and cutaneous lymphomas (108 [4.5%]). Risks were most strongly elevated for cancers associated with viruses, including Kaposi sarcoma (SIR, 20.5; 95% CI, 17.7-23.7), Merkel cell carcinoma (SIR, 16.2; 95% CI, 14.5-18.1), and extranodal natural killer/T-cell lymphoma (SIR, 44.3; 95% CI, 5.37-160). Risks were also significantly elevated for sebaceous carcinoma (SIR, 15.2; 95% CI, 13.0-17.7), anaplastic large cell lymphoma (SIR, 6.82; 95% CI, 4.53-9.85), and diffuse large B-cell lymphoma (SIR, 5.17; 95% CI, 3.28-7.76). Several characteristics were independently associated with greater risk for multiple skin cancer types, including male sex, older age at transplant, factors associated with UV radiation exposure (non-Hispanic White race and ethnicity, living in an area with higher UV radiation exposure, and posttransplant diagnosis of keratinocyte carcinoma), and increasing time since transplantation. Treatment with mammalian target of rapamycin inhibitors was associated with reduced melanoma incidence (incidence rate ratio, 0.75; 95% CI, 0.57-0.98). A total of 847 skin cancers (39.4%) occurred on the head and neck.
Conclusions and relevance: The findings of this cohort study suggest that viruses, UV radiation exposure, and immunosuppression are associated with the development of skin cancer in SOTRs. Certain high-risk subgroups may benefit from increased skin surveillance, and treatment with mammalian target of rapamycin inhibitors could be effective for melanoma chemoprevention in the transplant population.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
