

Characteristics and Outcomes of Type 2 Myocardial Infarction
- PMID: 35262640
- PMCID: PMC8908230
- DOI: 10.1001/jamacardio.2022.0043
Characteristics and Outcomes of Type 2 Myocardial Infarction
Abstract
Importance: In contrast to type 1 myocardial infarction (T1MI) caused by atherothrombosis, characteristics and outcomes of type 2 myocardial infarction (T2MI) caused by supply-demand mismatch are incompletely understood.
Objective: To explore the characteristics and outcomes of patients with T2MI compared with those with T1MI.
Design, Setting, and Participants: In a prospective, international, multicenter cohort study including 12 emergency departments (EDs) in 5 European countries, unselected patients presenting with acute chest discomfort were enrolled from April 2006 to April 2018. Follow-up was done by telephone or in written form 3, 12, and 24 months after hospital discharge. Data were analyzed from April 2006 to April 2020.
Interventions: The final diagnoses of T2MI and T1MI were centrally adjudicated according to the Fourth Universal Definition of Myocardial Infarction by 2 independent cardiologists, including the pathophysiological trigger of T2MI.
Main Outcomes and Measures: Patient characteristics and outcomes, including 2-year all-cause and cardiovascular mortality and future T2MI and T1MI events.
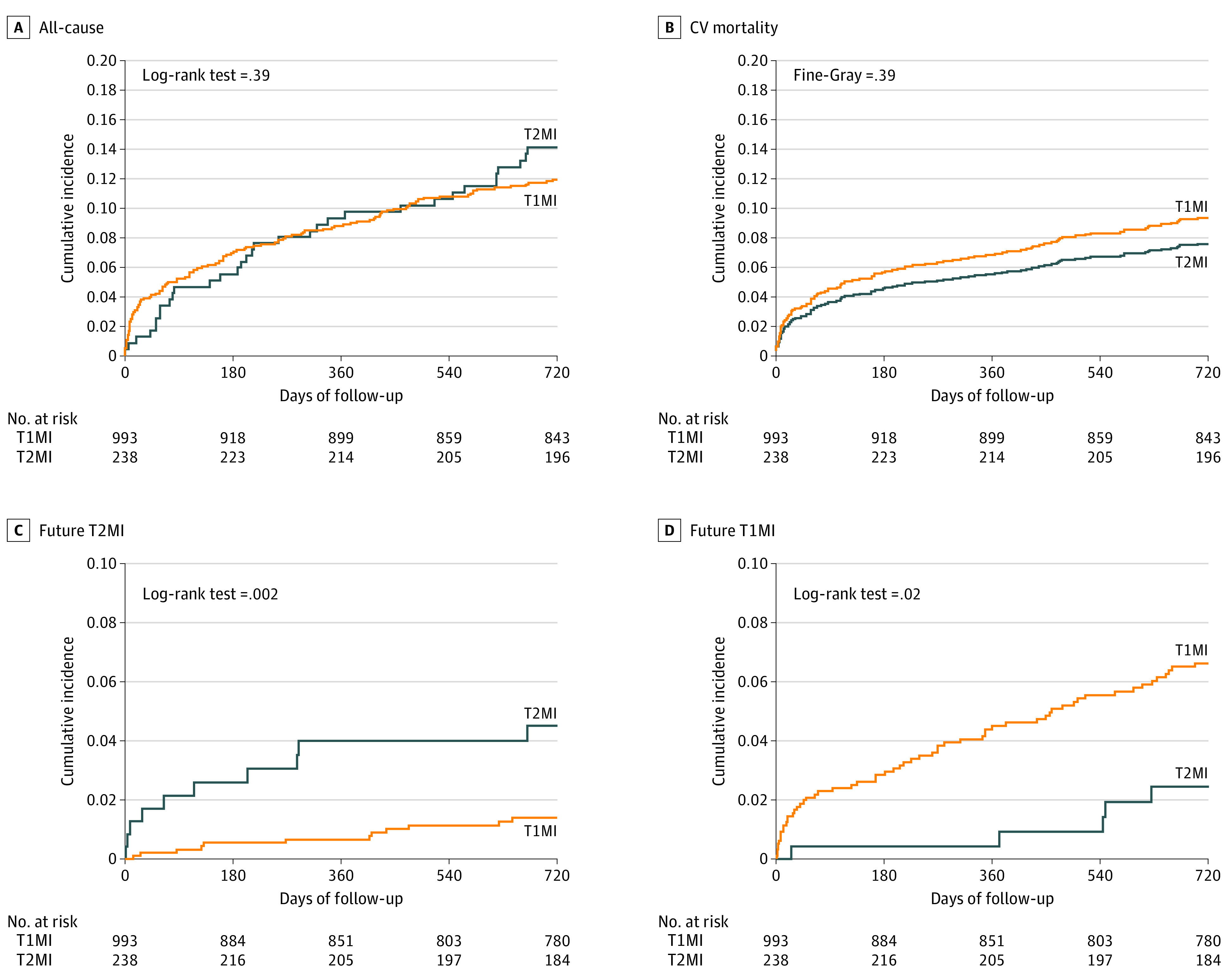
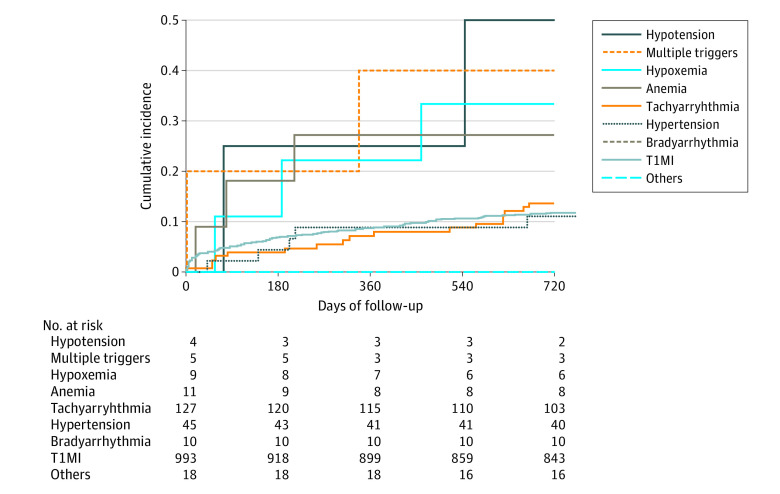
Results: Of 6253 included patients, 2078 (33.2%) were women, and the median (IQR) age was 61 (48-74) years. Among 6253 patients with acute chest discomfort, the final adjudicated diagnosis was T2MI in 251 patients (4.0%), with tachyarrhythmia and hypertension responsible for two-thirds of cases, and T1MI in 1027 patients (16.4%). All-cause and cardiovascular mortality were comparable at 2 years (T2MI: adjusted hazard ratio, 1.0; 95% CI, 0.7-1.5; T1MI: adjusted hazard ratio, 0.7; 95% CI, 0.4-1.1). Patients with tachyarrhythmia or hypertension as their underlying trigger of T2MI had a lower mortality compared with patients with hypotension, hypoxemia, or anemia. Future T2MI was more likely among patients with index T2MI compared with patients with index T1MI (hazard ratio, 3.2; 95% CI, 1.4-7.5). Similarly, future T1MI was more likely to occur among patients with index T1MI (hazard ratio, 3.0; 95% CI, 1.2-7.4).
Conclusions and Relevance: Among patients with T2MI, tachyarrhythmia and hypertension were responsible for more than two-thirds of T2MI cases. While T2MI and T1MI had comparable all-cause and cardiovascular mortality at 2 years, patients with tachyarrhythmia or hypertension as their underlying trigger of T2MI had a lower mortality compared with patients with hypotension, hypoxemia, or anemia. Future T2MI occurred 3-fold more frequently among patients with T2MI vs T1MI as the index event. Improved understanding of the specifics of patients with T2MI should help improve management strategies.
Conflict of interest statement
Figures
References
-
- Collet J-P, Thiele H, Barbato E, et al. ; ESC Scientific Document Group . 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent st-segment elevation: the Task Force for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2021;42(14):1289-1367. doi:10.1093/eurheartj/ehaa575 - DOI - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. ; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines . 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):362-425. doi:10.1161/CIR.0b013e3182742c84 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
