

Reducing ischemic kidney injury through application of a synchronization modulation electric field to maintain Na+/K+-ATPase functions
- PMID: 35263146
- PMCID: PMC9994383
- DOI: 10.1126/scitranslmed.abj4906
Reducing ischemic kidney injury through application of a synchronization modulation electric field to maintain Na+/K+-ATPase functions
Abstract
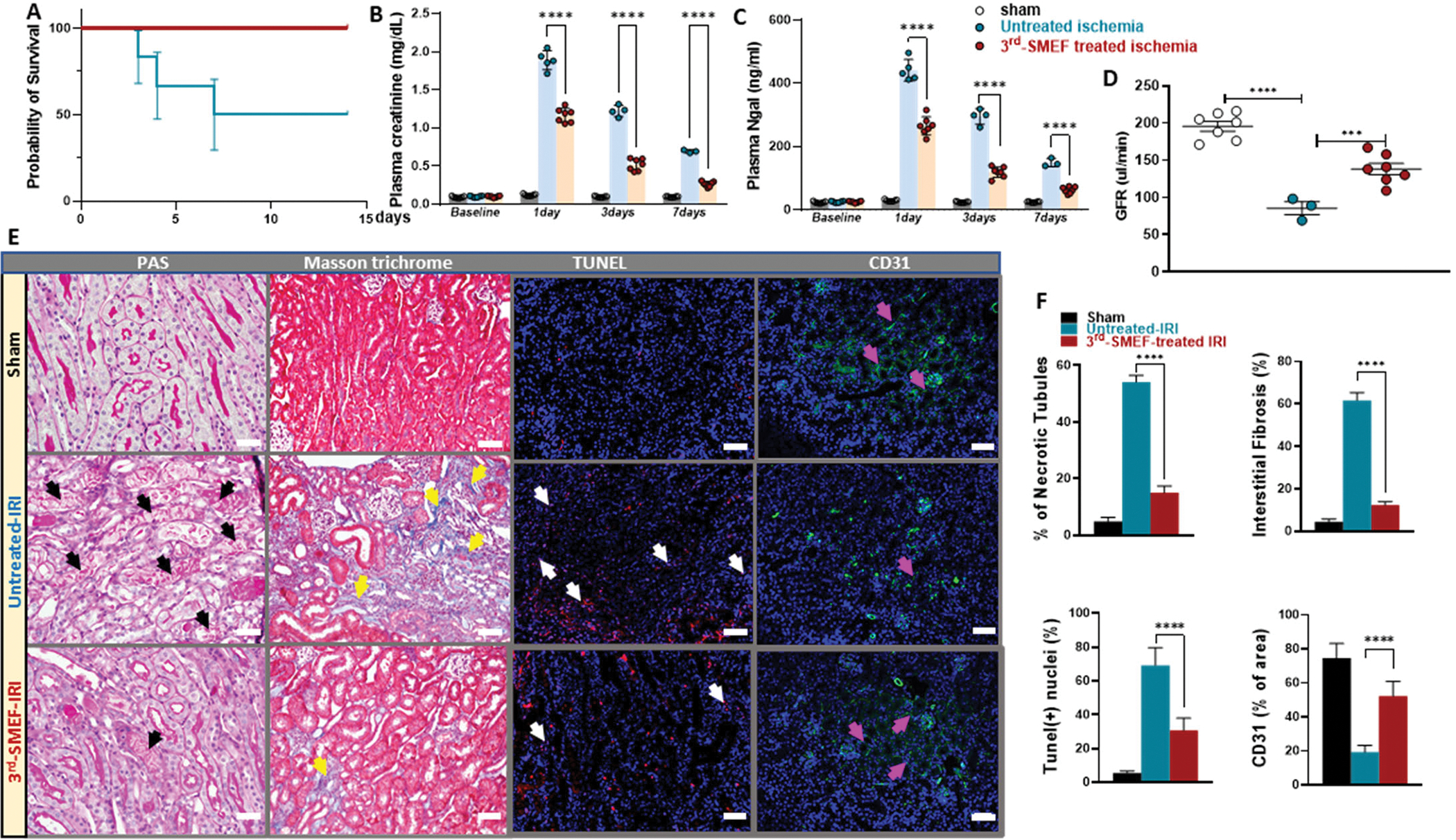
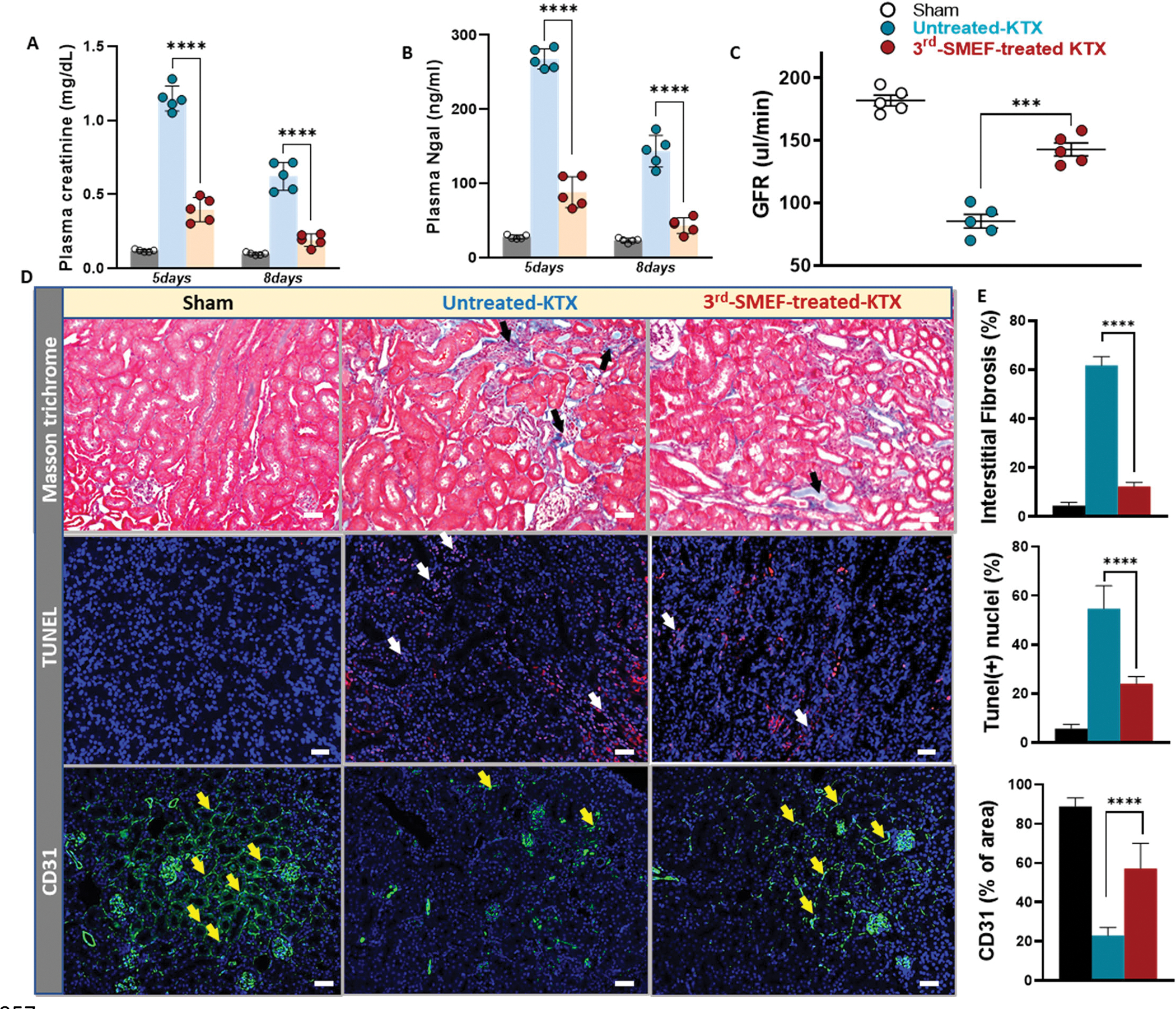
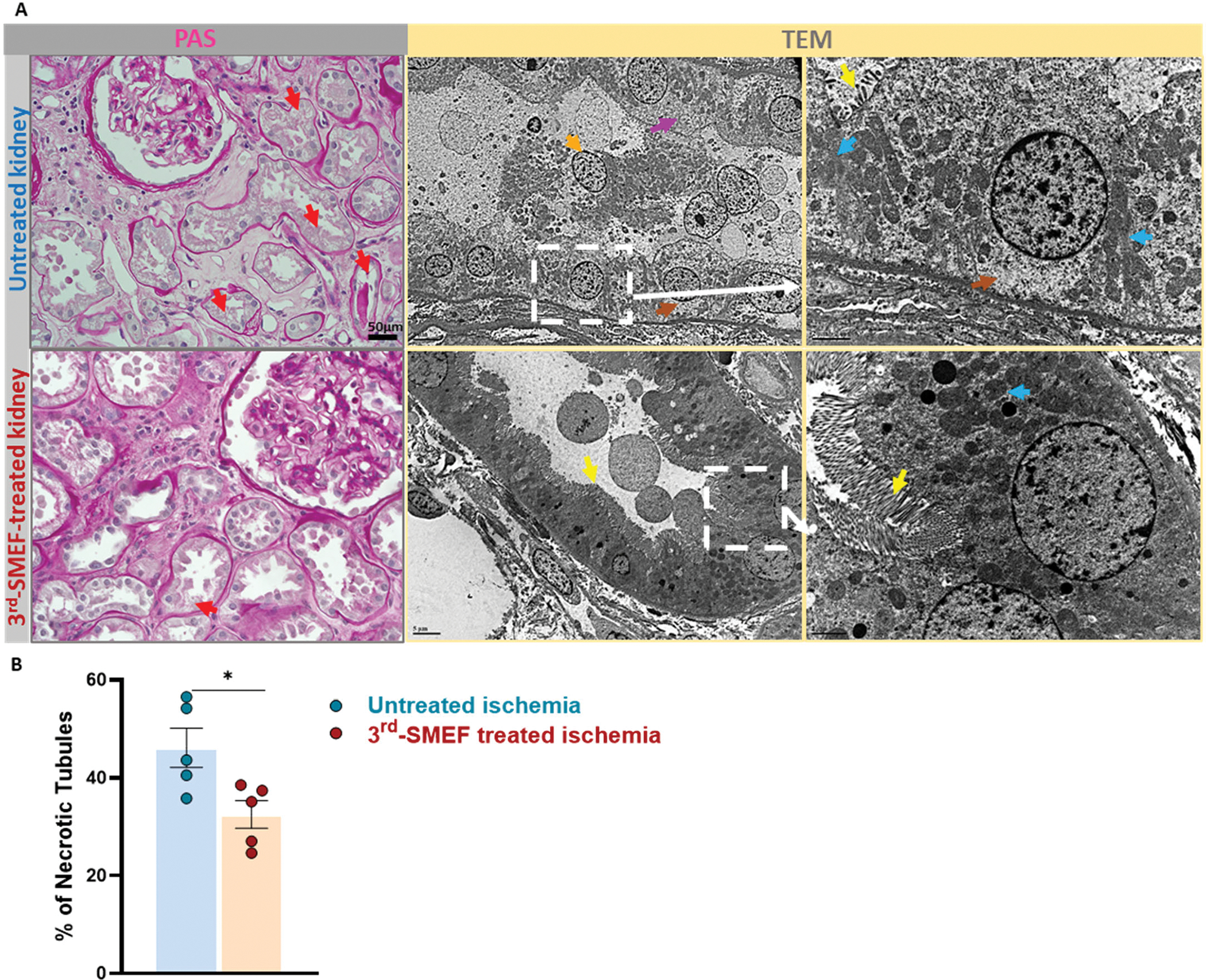
Renal ischemia-reperfusion injury is an important contributor to the development of delayed graft function after transplantation, which is associated with higher rejection rates and poorer long-term outcomes. One of the earliest impairments during ischemia is Na+/K+-ATPase (Na/K pump) dysfunction due to insufficient ATP supply, resulting in subsequent cellular damage. Therefore, strategies that preserve ATP or maintain Na/K pump function may limit the extent of renal injury during ischemia-reperfusion. Here, we applied a synchronization modulation electric field to activate Na/K pumps, thereby maintaining cellular functions under ATP-insufficient conditions. We tested the effectiveness of this technique in two models of ischemic renal injury: an in situ renal ischemia-reperfusion injury model (predominantly warm ischemia) and a kidney transplantation model (predominantly cold ischemia). Application of the synchronization modulation electric field to a renal ischemia-reperfusion injury mouse model preserved Na/K pump activity, thereby reducing kidney injury, as reflected by 40% lower plasma creatinine (1.17 ± 0.03 mg/dl) in the electric field-treated group as compared to the untreated control group (1.89 ± 0.06 mg/dl). In a mouse kidney transplantation model, renal graft function was improved by more than 50% with the application of the synchronization modulation electric field according to glomerular filtration rate measurements (85.40 ± 12.18 μl/min in the untreated group versus 142.80 ± 11.65 μl/min in the electric field-treated group). This technique for preserving Na/K pump function may have therapeutic potential not only for ischemic kidney injury but also for other diseases associated with Na/K pump dysfunction due to inadequate ATP supply.
Conflict of interest statement
Figures
Similar articles
-
Short communication: Ischemia increases cortical Na⁺,K⁺-ATPase activity (K-Pase) in a model of kidney auto-transplantation in the large white pig.Cell Mol Biol (Noisy-le-grand). 2014 Dec 30;60(6):16-9. Cell Mol Biol (Noisy-le-grand). 2014. PMID: 25553349
-
Effect of oxygen derived free radicals and glycine on sodium-potassium adenosine triphosphatase in the basolateral membrane of the kidney in ischemia-reperfusion.Saudi Med J. 2002 Nov;23(11):1380-5. Saudi Med J. 2002. PMID: 12506300
-
Cortical Na+,K+-ATPase activity, abundance and distribution after in vivo renal ischemia without reperfusion in rats.Nephron. 2001 Sep;89(1):82-9. doi: 10.1159/000046048. Nephron. 2001. PMID: 11528237
-
Modulation of pulmonary NA+ pump gene expression during cold storage and reperfusion.Transplantation. 2000 Oct 15;70(7):1016-20. doi: 10.1097/00007890-200010150-00005. Transplantation. 2000. PMID: 11045636
-
AMP-activated protein kinase as a target for preconditioning in transplantation medicine.Transplantation. 2010 Aug 27;90(4):353-8. doi: 10.1097/TP.0b013e3181e7a3aa. Transplantation. 2010. PMID: 20571465 Review.
Cited by
-
Roles of Akirin1 in early prediction and treatment of graft kidney ischemia‒reperfusion injury.Smart Med. 2024 Apr 2;3(2):e20230043. doi: 10.1002/SMMD.20230043. eCollection 2024 Jun. Smart Med. 2024. PMID: 39188701 Free PMC article.
-
Nephroprotective Effects of Cardamonin on Renal Ischemia Reperfusion Injury/UUO-Induced Renal Fibrosis.J Agric Food Chem. 2023 Sep 13;71(36):13284-13303. doi: 10.1021/acs.jafc.3c01880. Epub 2023 Aug 30. J Agric Food Chem. 2023. PMID: 37646396 Free PMC article.
-
Macula Densa Nitric Oxide Synthase 1 Controls Renin Release and Renin-Dependent Blood Pressure Changes.Discov Med. 2023 Aug;35(177):525-532. doi: 10.24976/Discov.Med.202335177.53. Discov Med. 2023. PMID: 37553306 Free PMC article.
-
Enhancing Liver Transplant Outcomes through Liver Precooling to Mitigate Inflammatory Response and Protect Mitochondrial Function.Biomedicines. 2024 Jul 4;12(7):1475. doi: 10.3390/biomedicines12071475. Biomedicines. 2024. PMID: 39062048 Free PMC article.
-
Small extracellular vesicles delivering lncRNA WAC-AS1 aggravate renal allograft ischemia‒reperfusion injury by inducing ferroptosis propagation.Cell Death Differ. 2023 Sep;30(9):2167-2186. doi: 10.1038/s41418-023-01198-x. Epub 2023 Aug 2. Cell Death Differ. 2023. PMID: 37532764 Free PMC article.
References
-
- Halloran PF, Aprile MA, Farewell V, Ludwin D, Smith EK, Tsai SY, Bear RA, Cole EH, Fenton SS, Cattran DC, Early function as the principal correlate of graft survival. A multivariate analysis of 200 cadaveric renal transplants treated with a protocol incorporating antilymphocyte globulin and cyclosporine. Transplantation 46, 223–228 (1988). - PubMed
-
- Womer KL, Vella JP, Sayegh MH, Chronic allograft dysfunction: mechanisms and new approaches to therapy. Semin. Nephrol 20, 126–147 (2000). - PubMed
-
- Nehus EJ, Devarajan P, Acute kidney injury: AKI in kidney transplant recipients--here to stay. Nat. Rev Nephrol 8, 198–199 (2012). - PubMed
-
- Daemen MA, de VB, Buurman WA, Apoptosis and inflammation in renal reperfusion injury. Transplantation 73, 1693–1700 (2002). - PubMed
-
- Cooper JE, Wiseman AC, Acute kidney injury in kidney transplantation. Curr. Opin. Nephrol. Hypertens 22, 698–703 (2013). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
