

Trends in Late Mortality and Life Expectancy After Autologous Blood or Marrow Transplantation Over Three Decades: A BMTSS Report
- PMID: 35263165
- PMCID: PMC9197350
- DOI: 10.1200/JCO.21.02372
Trends in Late Mortality and Life Expectancy After Autologous Blood or Marrow Transplantation Over Three Decades: A BMTSS Report
Abstract
Purpose: We determined trends in life expectancy and cause-specific late mortality after autologous blood or marrow transplantation (BMT) performed over a 30-year period, using the BMT Survivor Study.
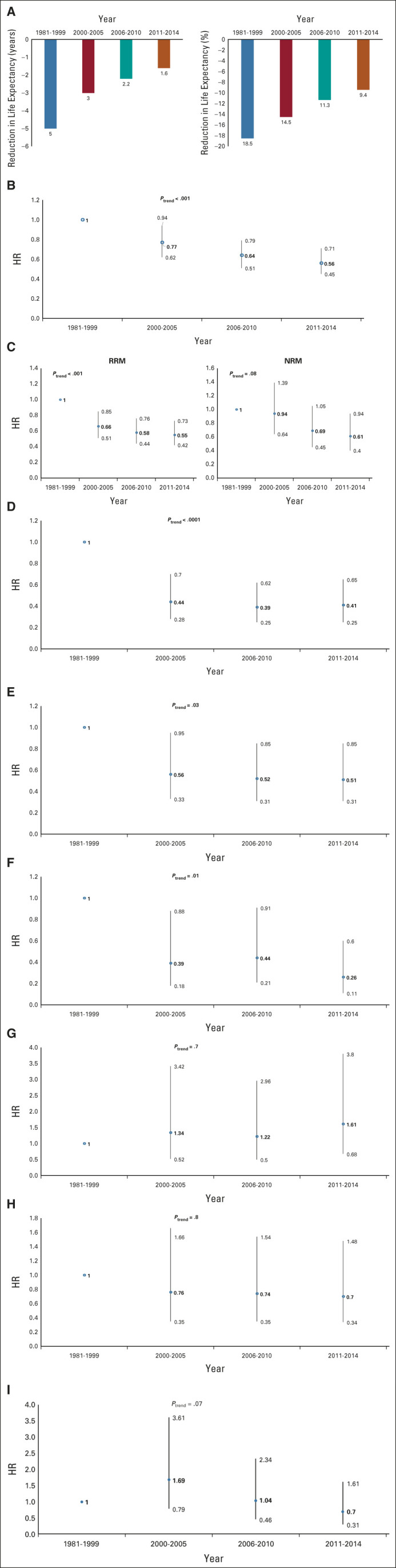
Methods: We constructed a cohort of 4,702 individuals with hematologic neoplasms who lived ≥ 2 years after autologous BMT performed between 1981 and 2014 at three transplant centers. The end of follow-up was April 19, 2021. The primary exposure variable was autologous BMT performed in four eras: 1981-1999; 2000-2005; 2006-2010; and 2011-2014. Vital status and cause of death were obtained from National Death Index Plus program and Accurinct databases.
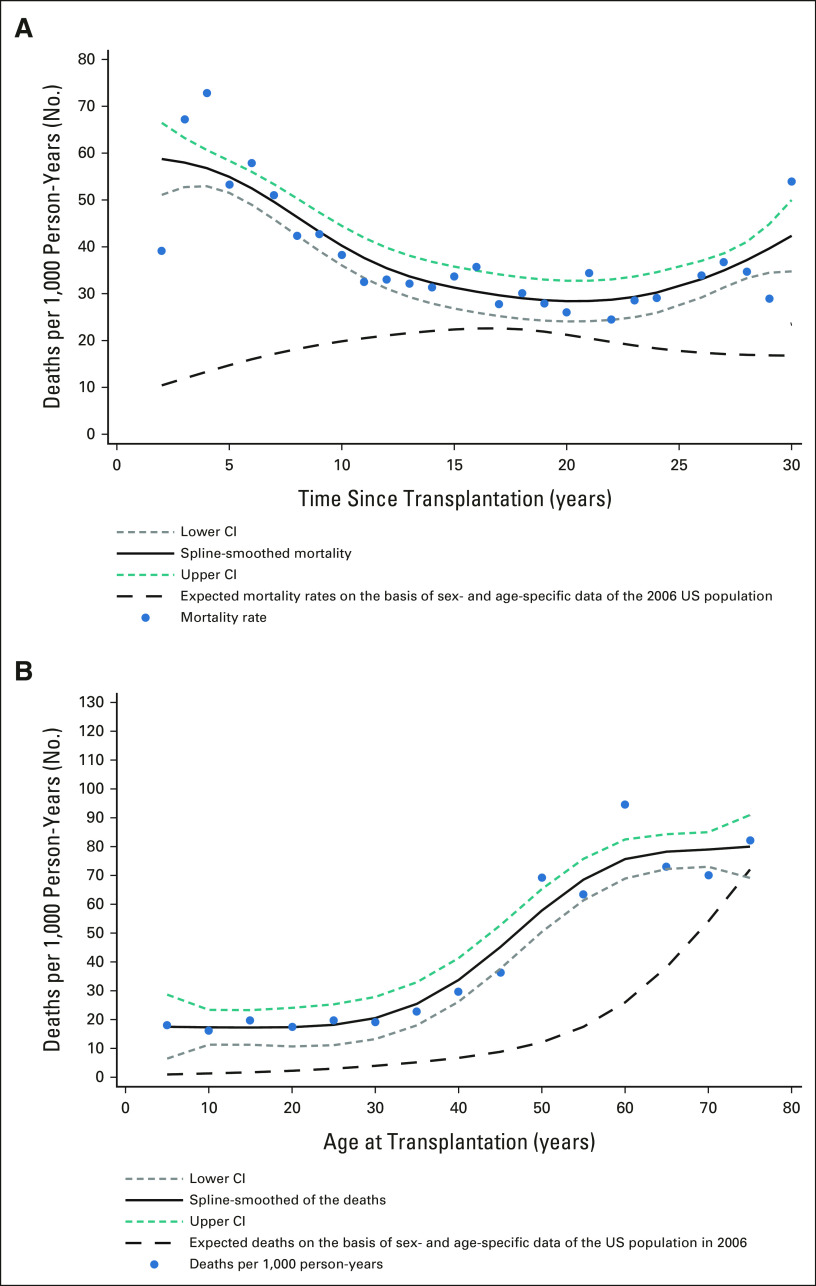
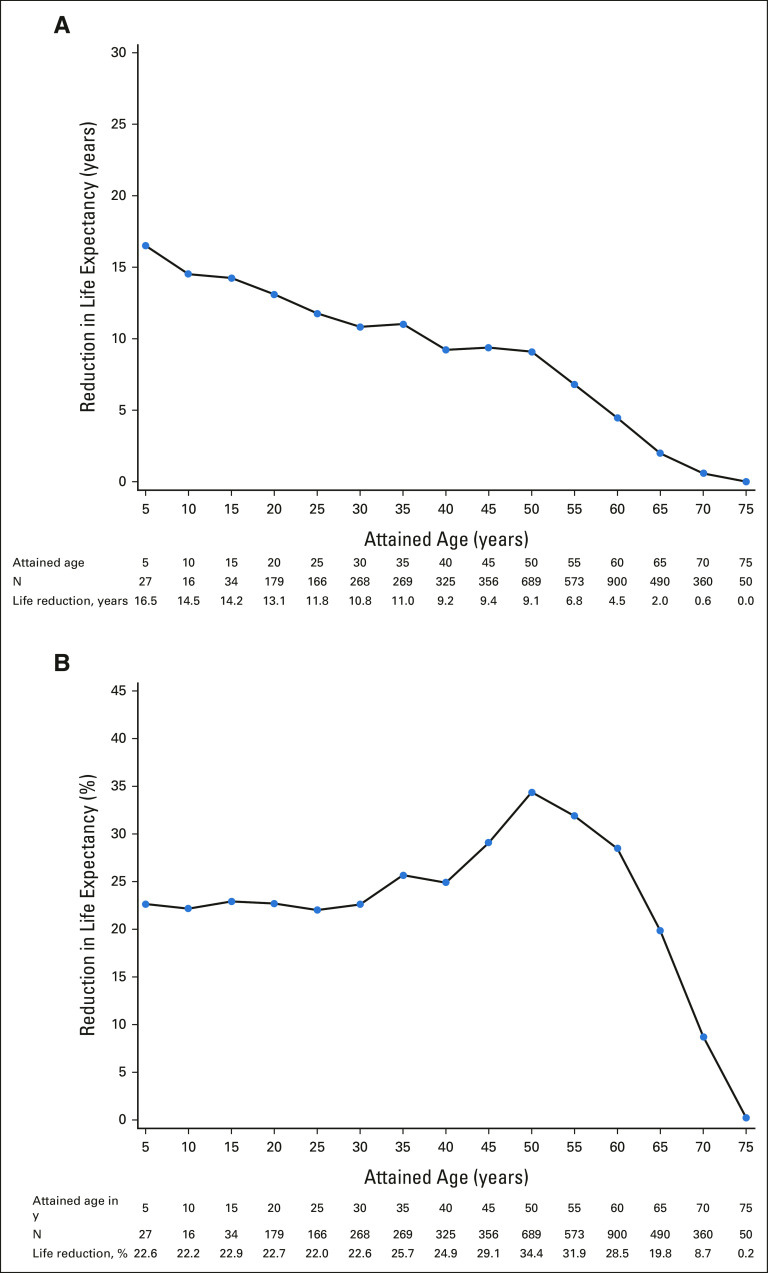
Results: The median age at BMT was 53 years (range, 0-78 years), 58.7% were male, 67.8% were non-Hispanic White, and 28.3% had undergone transplantation between 2011 and 2014. Autologous BMT recipients experienced a 7-year reduction in life expectancy. The adjusted hazard of 5-year all-cause mortality declined over the four eras (reference: 1981-1999; hazard ratio [HR]2000-2005 = 0.77; 95% CI, 0.62 to 0.94; HR2006-2010 = 0.64; 95% CI, 0.51 to 0.79; HR2011-2014 = 0.56; 95% CI, 0.45 to 0.71; Ptrend < .001), as did years of life lost (5.0 years to 1.6 years). The reduction in all-cause mortality was most pronounced among those transplanted for Hodgkin lymphoma or plasma cell dyscrasias, but was not observed among those transplanted for non-Hodgkin lymphoma or those conditioned with total-body irradiation. We also observed a decline in late deaths because of infection (Ptrend < .0001; primarily for BMTs before 2006) and subsequent neoplasms (Ptrend = .03; confined to decline in therapy-related myeloid neoplasm-related mortality) but not because of cardiovascular or renal disease.
Conclusion: Late mortality among autologous BMT recipients has declined over a 30-year period. However, ongoing efforts are needed to mitigate development of infections, subsequent neoplasms, and cardiovascular and renal disease to further reduce late mortality.
Conflict of interest statement
Figures
Comment in
-
Living Long and Well After an Autograft.J Clin Oncol. 2022 Jun 20;40(18):1971-1975. doi: 10.1200/JCO.22.00302. Epub 2022 May 5. J Clin Oncol. 2022. PMID: 35512253 No abstract available.
References
-
- Jantunen E, Varmavuo V, Pelkonen J, et al. Importance of early immune recovery after autologous hematopoietic cell transplantation in lymphoma patients Leuk Lymphoma 602115–21212019 - PubMed
-
- Jantunen E, Itälä M, Lehtinen T, et al. Early treatment-related mortality in adult autologous stem cell transplant recipients: A nation-wide survey of 1482 transplanted patients Eur J Haematol 76245–2502006 - PubMed
-
- André M, Henry-Amar M, Blaise D, et al. Treatment-related deaths and second cancer risk after autologous stem-cell transplantation for Hodgkin's disease Blood 921933–19401998 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
