

Impact of Circulating Tumor DNA-Based Detection of Molecular Residual Disease on the Conduct and Design of Clinical Trials for Solid Tumors
- PMID: 35263168
- PMCID: PMC8926064
- DOI: 10.1200/PO.21.00181
Impact of Circulating Tumor DNA-Based Detection of Molecular Residual Disease on the Conduct and Design of Clinical Trials for Solid Tumors
Erratum in
-
Erratum.JCO Precis Oncol. 2022 Apr;6:e2200193. doi: 10.1200/PO.22.00193. JCO Precis Oncol. 2022. PMID: 35483001 Free PMC article. No abstract available.
Abstract
Purpose: Earlier detection of cancer recurrence using circulating tumor DNA (ctDNA) to detect molecular residual disease (MRD) has the potential to dramatically affect cancer management. We review evidence supporting the use of ctDNA as a biomarker for detection of MRD and highlight the potential impact that ctDNA testing could have on the conduct of clinical trials.
Methods: We searched the literature using MEDLINE (via PubMed) for articles from January 1, 2000, focusing on studies that assessed ctDNA as a predictor of cancer recurrence. Broadly focused searches on ctDNA and cancer were also performed to provide additional background information. www.clinialtrials.gov was searched to identify trials that incorporate ctDNA testing.
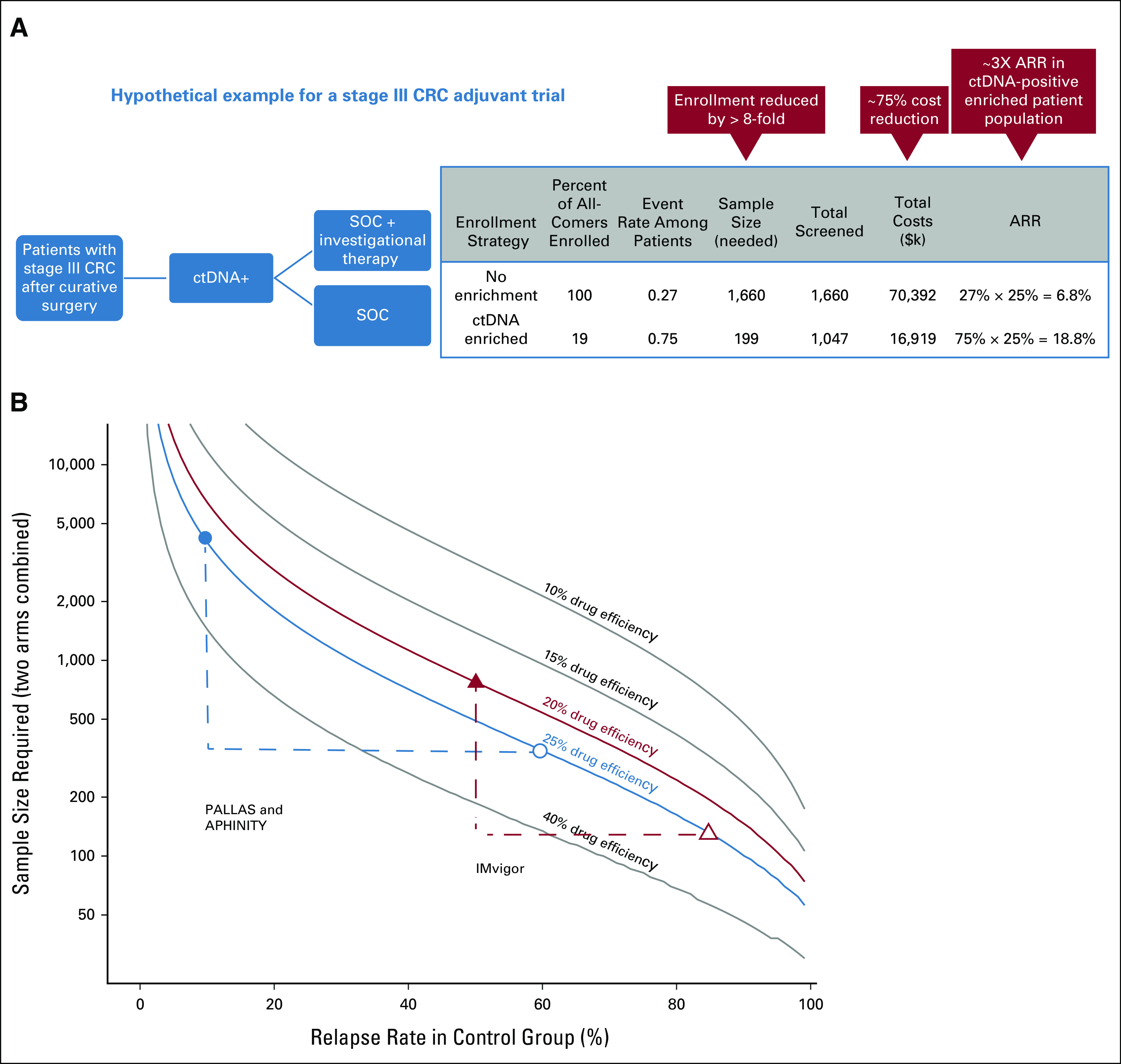
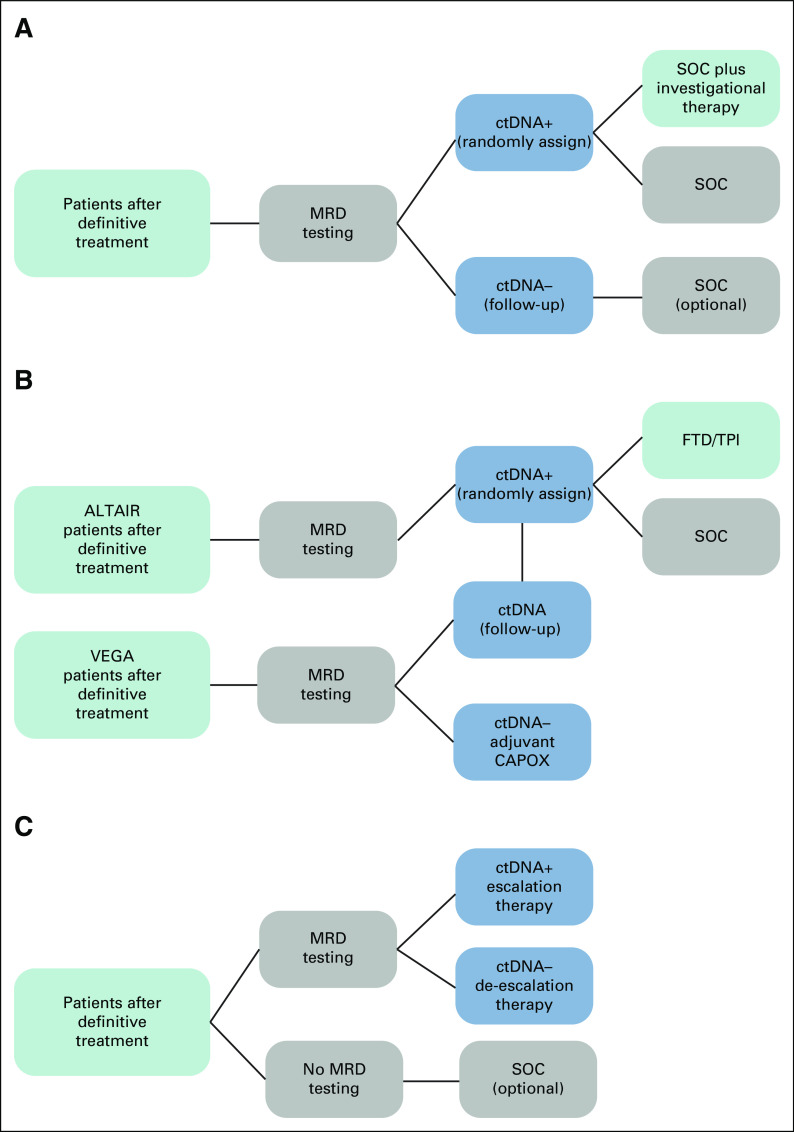
Results: Numerous studies across different cancer types indicate that ctDNA-based MRD detection predicts recurrence with high sensitivity and specificity, and with lead times that precede standard imaging by up to 12 months. Recently, ctDNA testing has started being used to enroll MRD-positive patients at high risk of recurrence into trials, promising gains in statistical power that allow clinical utility to be demonstrated with smaller cohorts. Trials where ctDNA testing based-MRD detection is used to stratify patients into low or high-risk categories for treatment assignment are also ongoing. In addition, there is increasing evidence supporting the use of ctDNA dynamics or clearance as a surrogate end point, which could significantly reduce trial duration.
Conclusion: ctDNA-based trial enrichment across many cancers seems likely to become increasingly common for cost- and time-reduction benefits. Trial efficiency could also benefit from using ctDNA as a surrogate end point, leading to accelerated approval of new therapeutics. A clear demonstration of efficacy from trials that use ctDNA-based MRD detection to assign treatment could transform clinical practice.
Conflict of interest statement
Figures
Comment in
-
Spontaneous Fluctuations of Tumor-Informed Circulating Tumor DNA at Low Levels.JCO Precis Oncol. 2022 Jul;6:e2200177. doi: 10.1200/PO.22.00177. JCO Precis Oncol. 2022. PMID: 35834756 No abstract available.
-
Reply to F. Dayyani et al.JCO Precis Oncol. 2022 Jul;6:e2200275. doi: 10.1200/PO.22.00275. JCO Precis Oncol. 2022. PMID: 35834757 No abstract available.
References
-
- Mandel P, Metais P. Les acides nucléiques du plasma sanguin chez l’ homme. C R Seances Soc Biol Fil. 1948;142:241–243. - PubMed
-
- Sorenson GD, Pribish DM, Valone FH, et al. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol Biomarkers Prev. 1994;3:67–71. - PubMed
-
- Vasioukhin V, Anker P, Maurice P, et al. Point mutations of the N-ras gene in the blood plasma DNA of patients with myelodysplastic syndrome or acute myelogenous leukaemia. Br J Haematol. 1994;86:774–779. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
