

Neurobiological and pharmacological arguments for customization of cognitive behavioral psychotherapy in the treatment of major depressive disorder
- PMID: 35263410
- PMCID: PMC9019623
- DOI: 10.47162/RJME.62.3.19
Neurobiological and pharmacological arguments for customization of cognitive behavioral psychotherapy in the treatment of major depressive disorder
Abstract
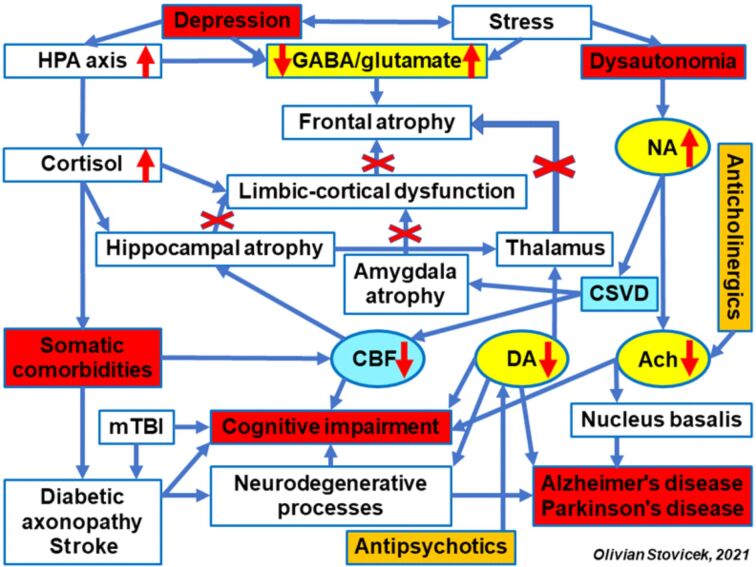
Introduction: Depression represents a public health issue because it significantly increases the risk of disabilities and premature mortality, decreases the quality of life, and increases the costs of care. The incomplete remissions favor the aggravation of neurobiological dysfunctions and pathogenesis of severe somatic comorbidities. The etiopathogenic mechanisms of depression are complex and involve multisystemic risk factors (genetic, neuroanatomic, neurobiochemical, neuroendocrine and psychosocial). Cognitive behavioral therapy (CBT) is used in all the stages of depression, as independent therapeutic method or as support of pharmacotherapy.
Patients, materials and methods: This study has evaluated the therapeutic response of depression in M (medication) group with 136 patients under pharmacotherapy, compared with P (psychotherapy and medication) group with 137 patients treated simultaneously with medication and CBT, and the factors that can improve therapeutic management.
Results: Patients with depression had predominantly a reactive onset, recurrent evolution of at least four episodes, and frequent somatic comorbidities. After treatment, a significant improvement of depressive symptomatology was recorded especially in M group (72.06%), compared to P group (88.32%), p<0.01, as well as a significant difference in regaining functional skills (69.12% - M group, 93.43% - P group; p<0.001). The therapeutic response was significantly correlated with age (p<0.01), social-economical involvement and education level.
Conclusions: CBT demonstrated efficiency in the treatment of major depressive disorder in association with pharmacotherapy. The therapeutic approach should rely on the pathogenic biological models that would highlight the prediction indicators for the therapeutic response and for the evolution of depression, as well as considering the psychological profile of each patient.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
Similar articles
-
Internet-Delivered Cognitive Behavioural Therapy for Major Depression and Anxiety Disorders: A Health Technology Assessment.Ont Health Technol Assess Ser. 2019 Feb 19;19(6):1-199. eCollection 2019. Ont Health Technol Assess Ser. 2019. PMID: 30873251 Free PMC article.
-
Psychotherapy for Major Depressive Disorder and Generalized Anxiety Disorder: A Health Technology Assessment.Ont Health Technol Assess Ser. 2017 Nov 13;17(15):1-167. eCollection 2017. Ont Health Technol Assess Ser. 2017. PMID: 29213344 Free PMC article. Review.
-
Psychosocial interventions for preventing and treating depression in dialysis patients.Cochrane Database Syst Rev. 2019 Dec 2;12(12):CD004542. doi: 10.1002/14651858.CD004542.pub3. Cochrane Database Syst Rev. 2019. PMID: 31789430 Free PMC article.
-
Neurobiological mechanisms of exercise and psychotherapy in depression: The SPeED study-Rationale, design, and methodological issues.Clin Trials. 2018 Feb;15(1):53-64. doi: 10.1177/1740774517729161. Epub 2017 Sep 14. Clin Trials. 2018. PMID: 28905640
-
Temporal and specific pathways of change in cognitive behavioral therapy (CBT) and interpersonal psychotherapy (IPT) for depression.Behav Res Ther. 2022 Apr;151:104010. doi: 10.1016/j.brat.2021.104010. Epub 2021 Nov 27. Behav Res Ther. 2022. PMID: 35228163 Clinical Trial.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. . Lancet. 2018;2019;392393(10159)(10190):1789–1858. e44–e44. - PMC - PubMed
-
- World Health Organization (WHO) Depression and other common mental disorders global health estimates.Document No. WHO/MSD/MER/2017.2, License: CC BY-NC-SA 3.0 IGO. Geneva, Switzerland: WHO; 2017. https://apps.who.int/iris/handle/10665/254610
MeSH terms
LinkOut - more resources
Full Text Sources
