Effect of modified care bundle for prevention of ventilator-associated pneumonia in critically-ill neurosurgical patients
- PMID: 35263824
- PMCID: PMC8907469
- DOI: 10.4266/acc.2021.00983
Effect of modified care bundle for prevention of ventilator-associated pneumonia in critically-ill neurosurgical patients
Abstract
Background: Care bundles for ventilator-associated pneumonia (VAP) have been shown to minimize the rate of VAP in critically ill patients. Standard care bundles may need to be modified in resource-constrained situations. The goal of this study was to see if our modified VAP-care bundles lowered the risk of VAP in neurosurgical patients.
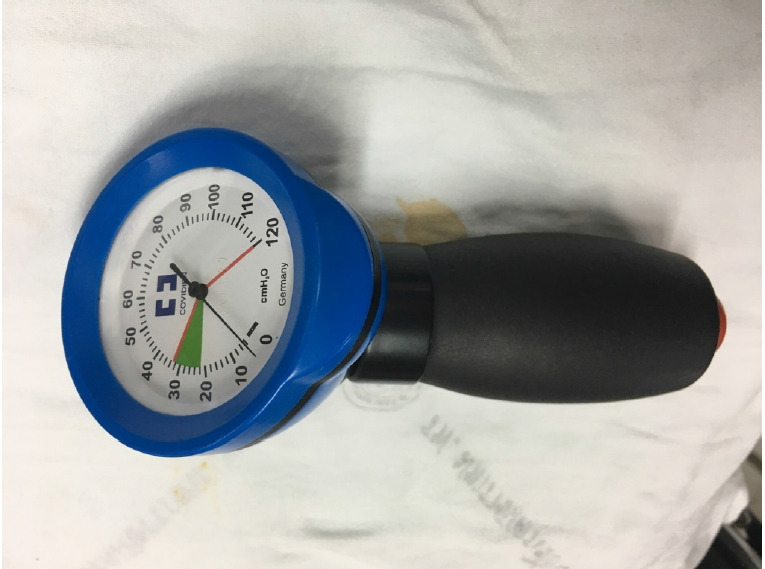
Methods: A prospective cohort study was conducted in mechanically ventilated neurosurgical patients. The VAP bundle was adjusted in the cohort group by increasing the frequency of intermittent endotracheal tube cuff pressure monitoring to six times a day while reducing oral care with 0.12% chlorhexidine to three times a day. The rate of VAP was compared to the historical control group.
Results: A total of 146 and 145 patients were enrolled in control and cohort groups, respectively. The mean age of patients was 52±16 years in both groups (P=0.803). The admission Glasgow coma scores were 7.79±2.67 and 7.80±2.77 in control and cohort group, respectively (P=0.969). VAP was found in nine patients in control group but only one patient in cohort group. The occurrence rate of VAP was significantly reduced in cohort group compared to control group (0.88/1,000 vs. 6.84/1,000 ventilator days, P=0.036).
Conclusions: The modified VAP bundle is effective in lowering the VAP rate in critically ill neurosurgical patients. It requires low budget and manpower and can be employed in resource-constrained settings.
Keywords: chlorhexidine; critical care; intubation; neurosurgery; oral hygiene; ventilator-associated pneumonia.
Conflict of interest statement
Similar articles
-
[Ventilator bundle guided by context of JCI settings can effectively reduce the morbidity of ventilator-associated pneumonia].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jul;29(7):624-628. doi: 10.3760/cma.j.issn.2095-4352.2017.07.010. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28743340 Chinese.
-
Assessment of the effectiveness of a ventilator associated pneumonia prevention bundle that contains endotracheal tube with subglottic drainage and cuff pressure monitorization.Braz J Infect Dis. 2017 May-Jun;21(3):276-281. doi: 10.1016/j.bjid.2017.01.002. Epub 2017 Feb 11. Braz J Infect Dis. 2017. PMID: 28193455 Free PMC article. Clinical Trial.
-
The impact of implementing multifaceted interventions on the prevention of ventilator-associated pneumonia.Am J Infect Control. 2016 Mar 1;44(3):320-6. doi: 10.1016/j.ajic.2015.09.025. Am J Infect Control. 2016. PMID: 26940595
-
The Impact of Care Bundles on Ventilator-Associated Pneumonia (VAP) Prevention in Adult ICUs: A Systematic Review.Antibiotics (Basel). 2023 Jan 20;12(2):227. doi: 10.3390/antibiotics12020227. Antibiotics (Basel). 2023. PMID: 36830138 Free PMC article. Review.
-
Bundles to prevent ventilator-associated pneumonia: how valuable are they?Curr Opin Infect Dis. 2009 Apr;22(2):159-66. doi: 10.1097/QCO.0b013e3283295e7b. Curr Opin Infect Dis. 2009. PMID: 19276975 Review.
References
-
- Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest. 2002;122:2115–21. - PubMed
-
- Craven DE. Epidemiology of ventilator-associated pneumonia. Chest. 2000;117(4 Suppl 2):186S–187S. - PubMed
-
- Martin-Loeches I, Rodriguez AH, Torres A. New guidelines for hospital-acquired pneumonia/ventilator-associated pneumonia: USA vs. Europe. Curr Opin Crit Care. 2018;24:347–52. - PubMed
-
- Triamvisit S, Maneewan C, Bunturat P, Wongprasert W, Limpassatan K, Kasatpibal N, et al. Results of an evidence-based care bundle for reducing ventilator-associated pneumonia (VAP) in neurosurgical patients. J Med Assoc Thai. 2016;99:1014–9. - PubMed
LinkOut - more resources
Full Text Sources