

Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: prospective observational study
- PMID: 35264324
- PMCID: PMC8905308
- DOI: 10.1136/bmj-2021-069761
Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: prospective observational study
Abstract
Objectives: To characterize the clinical severity of covid-19 associated with the alpha, delta, and omicron SARS-CoV-2 variants among adults admitted to hospital and to compare the effectiveness of mRNA vaccines to prevent hospital admissions related to each variant.
Design: Case-control study.
Setting: 21 hospitals across the United States.
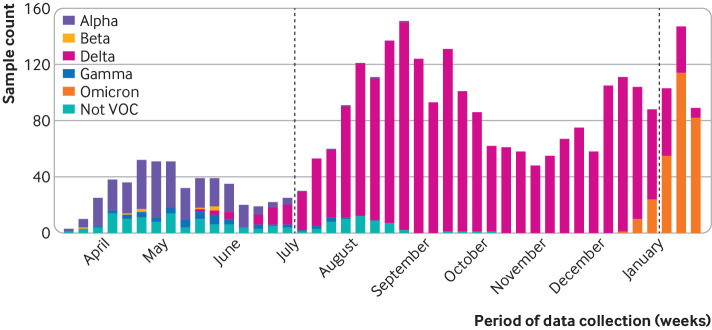
Participants: 11 690 adults (≥18 years) admitted to hospital: 5728 with covid-19 (cases) and 5962 without covid-19 (controls). Patients were classified into SARS-CoV-2 variant groups based on viral whole genome sequencing, and, if sequencing did not reveal a lineage, by the predominant circulating variant at the time of hospital admission: alpha (11 March to 3 July 2021), delta (4 July to 25 December 2021), and omicron (26 December 2021 to 14 January 2022).
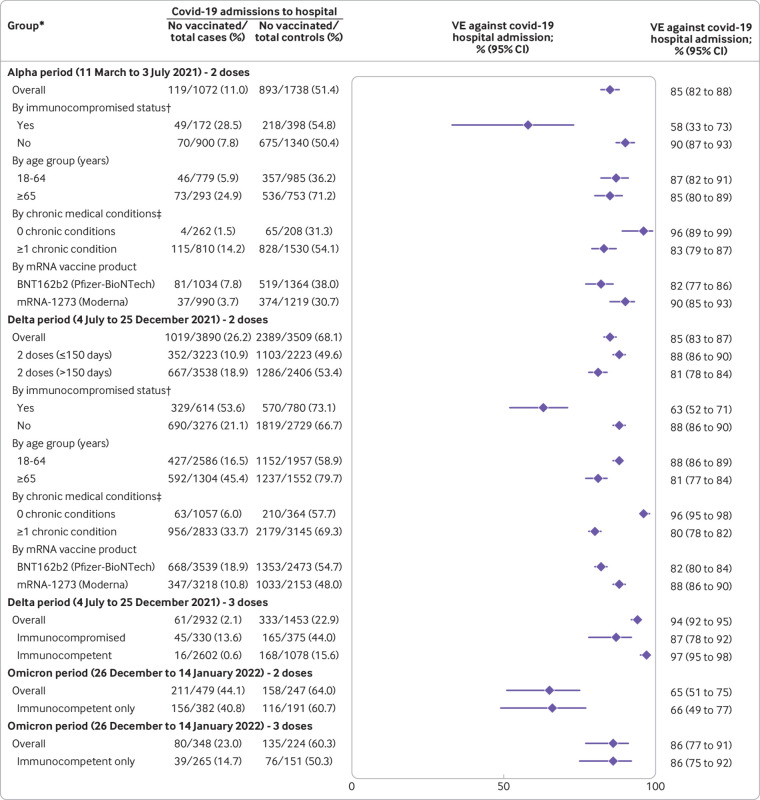
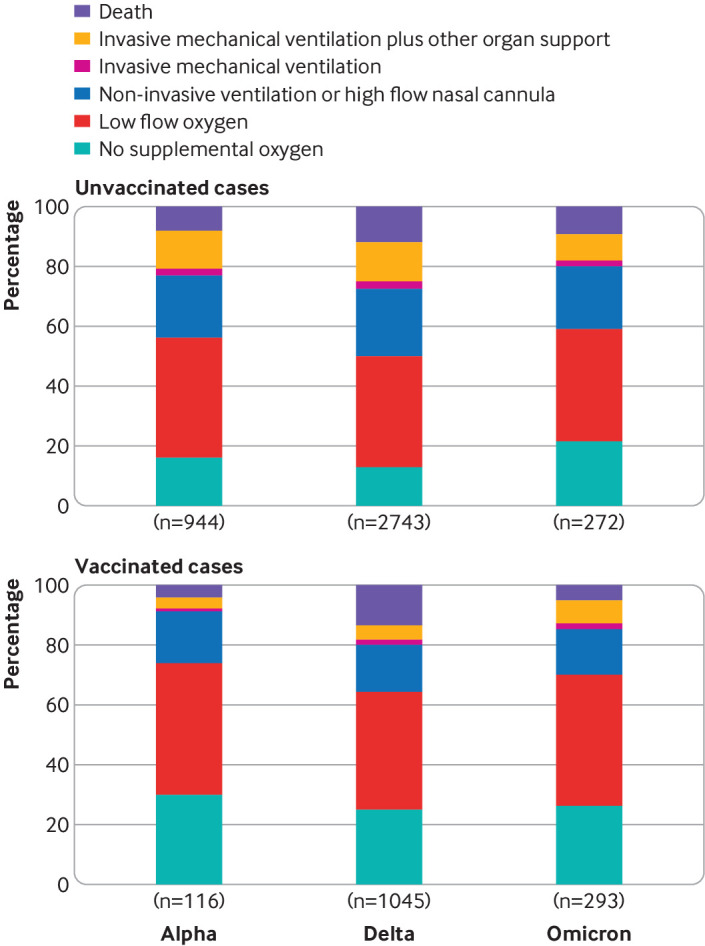
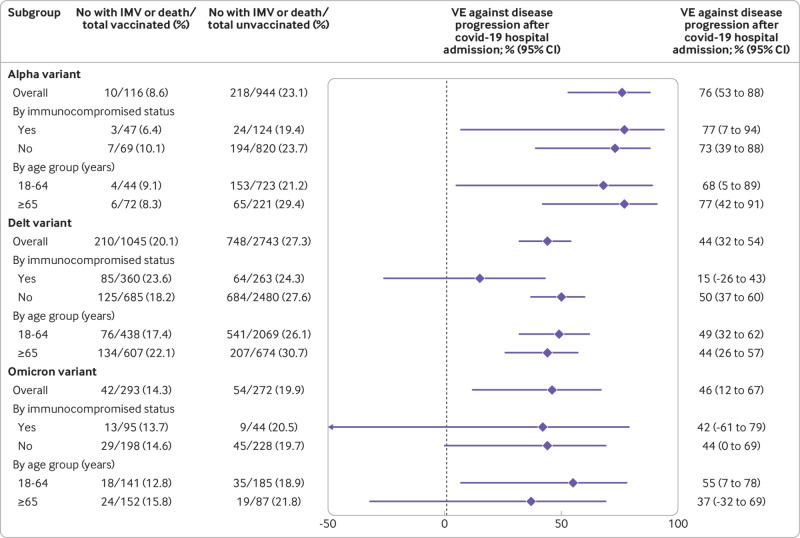
Main outcome measures: Vaccine effectiveness calculated using a test negative design for mRNA vaccines to prevent covid-19 related hospital admissions by each variant (alpha, delta, omicron). Among patients admitted to hospital with covid-19, disease severity on the World Health Organization's clinical progression scale was compared among variants using proportional odds regression.
Results: Effectiveness of the mRNA vaccines to prevent covid-19 associated hospital admissions was 85% (95% confidence interval 82% to 88%) for two vaccine doses against the alpha variant, 85% (83% to 87%) for two doses against the delta variant, 94% (92% to 95%) for three doses against the delta variant, 65% (51% to 75%) for two doses against the omicron variant; and 86% (77% to 91%) for three doses against the omicron variant. In-hospital mortality was 7.6% (81/1060) for alpha, 12.2% (461/3788) for delta, and 7.1% (40/565) for omicron. Among unvaccinated patients with covid-19 admitted to hospital, severity on the WHO clinical progression scale was higher for the delta versus alpha variant (adjusted proportional odds ratio 1.28, 95% confidence interval 1.11 to 1.46), and lower for the omicron versus delta variant (0.61, 0.49 to 0.77). Compared with unvaccinated patients, severity was lower for vaccinated patients for each variant, including alpha (adjusted proportional odds ratio 0.33, 0.23 to 0.49), delta (0.44, 0.37 to 0.51), and omicron (0.61, 0.44 to 0.85).
Conclusions: mRNA vaccines were found to be highly effective in preventing covid-19 associated hospital admissions related to the alpha, delta, and omicron variants, but three vaccine doses were required to achieve protection against omicron similar to the protection that two doses provided against the delta and alpha variants. Among adults admitted to hospital with covid-19, the omicron variant was associated with less severe disease than the delta variant but still resulted in substantial morbidity and mortality. Vaccinated patients admitted to hospital with covid-19 had significantly lower disease severity than unvaccinated patients for all the variants.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare the following. This study was funded by the US Centers for Disease Control and Prevention (CDC). ASL reports consultant fees from Sanofi and fees from Roche for membership on a trial steering committee. JDC reports grant support from CDC and National Institutes of Health (NIH). MG reports grant support from CDC. AAG reports grant support from CDC, NIH, Department of Defense (DoD), and an investigator initiated grant support from AbbVie and Faron Pharmaceuticals. HKT reports a grant from CDC. JDC reports a grant from the NIH (K23HL153584). DCF reports consultant fees from Cytovale and membership on a Medpace data safety monitoring board (DSMB). DNH reports a contract from CDC (via subcontract with Vanderbilt University Medical Center) and salary support from Incyte, EMPACT Precision Medicine, and the Marcus Foundation. MCE reports talks on nutrition in covid-19 pneumonia at the Nutritional Science and Practice Conference sponsored by Abbott Laboratories. MNG reports grant support from CDC, funding from the National Heart, Lung, and Blood Institute, and fees for participating on a DSMB for Regeneron. IDP reports grants from CDC, NIH, Intermountain Research and Medical Foundation, and Janssen Pharmaceuticals, institutional fees from Asahi Kasei Pharma and from Regeneron. SMB reports grants from CDC, Sedana, Janssen, NIH, and DoD; fees from Hamilton for chairing a DSMB; institutional fees from Faron; book royalties from Oxford University and Brigham Young University; and personal fees from New York University for service on a DSMB. ETM reports a grant from Merck for unrelated work. AK reports grants from Gilead, Ely Lily, United Therapeutics, Johnson and Johnson (Actelion), Liquidia Pharmaceuticals, and 4D Medical. SYC was a speaker for La Jolla Pharmaceuticals and a consultant for PureTech Health. JHK reports grant support from NIH/National Institute of Allergy and Infectious Diseases (1K23 AI137321-01A1). NH reports grants from CDC, Sanofi, and Quidel. CGG reports consultant fees from Pfizer, Merck, and Sanofi-Pasteur and grants from Campbell Alliance/Syneos Health, CDC, NIH, Food and Drug Administration, Agency for Healthcare Research and Quality, and Sanofi. TR reports grant support from CDC. CJL reports grants from CDC, NIH, DoD, and the Marcus Foundation; organizational contract fees from bioMerieux, Endpoint, and Entegrion; and a patent issued to Cincinnati Children’s Hospital Medical Center for risk stratification in sepsis and septic shock. WHS reports grant funding from CDC for this work, grants and consultant fees from Merck outside this work, and consultant fees from Aerpio Pharmaceuticals outside this work.
Figures
Update of
-
Clinical Severity and mRNA Vaccine Effectiveness for Omicron, Delta, and Alpha SARS-CoV-2 Variants in the United States: A Prospective Observational Study.medRxiv [Preprint]. 2022 Feb 7:2022.02.06.22270558. doi: 10.1101/2022.02.06.22270558. medRxiv. 2022. Update in: BMJ. 2022 Mar 9;376:e069761. doi: 10.1136/bmj-2021-069761. PMID: 35169811 Free PMC article. Updated. Preprint.
References
-
- Tracking SARS-CoV-2 variants. https://www.who.int/health-topics/typhoid/tracking-SARS-CoV-2-variants (accessed 26 Oct 2021).
-
- GISAID - hCov19 Variants. https://www.gisaid.org/hcov19-variants/ (accessed 26 Oct 2021).
-
- Twohig KA, Nyberg T, Zaidi A, et al. COVID-19 Genomics UK (COG-UK) consortium . Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: a cohort study. Lancet Infect Dis 2022;22:35-42. 10.1016/S1473-3099(21)00475-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous