

Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, non-inferiority trial
- PMID: 35264408
- PMCID: PMC8905684
- DOI: 10.1136/bmj-2021-0068229
Alternative to prophylactic antibiotics for the treatment of recurrent urinary tract infections in women: multicentre, open label, randomised, non-inferiority trial
Abstract
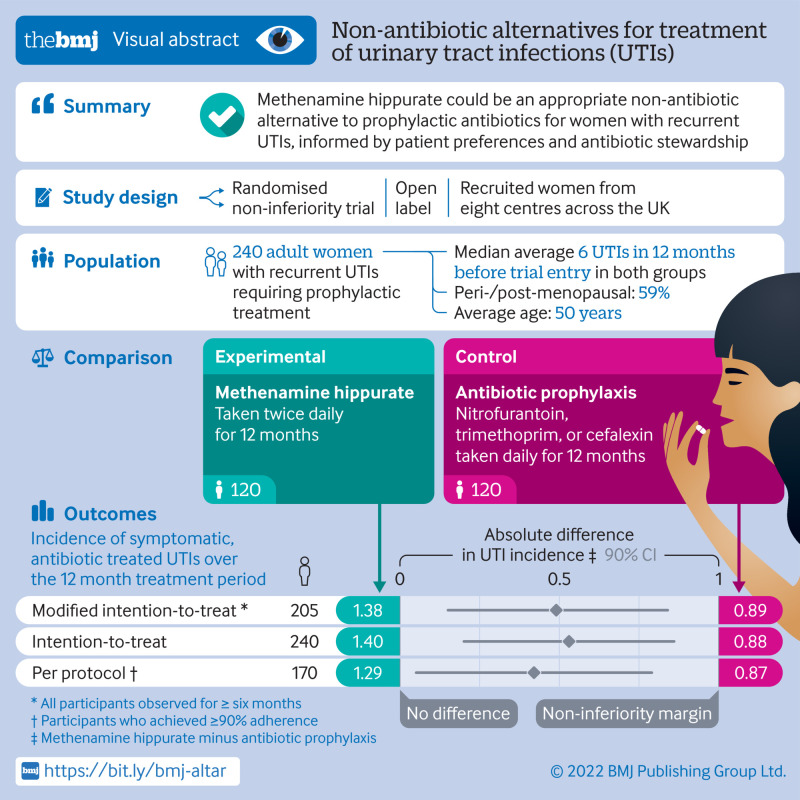
Objective: To test and compare the efficacy of methenamine hippurate for prevention of recurrent urinary tract infections with the current standard prophylaxis of daily low dose antibiotics.
Design: Multicentre, open label, randomised, non-inferiority trial.
Setting: Eight centres in the UK, recruiting from June 2016 to June 2018.
Participants: Women aged ≥18 years with recurrent urinary tract infections, requiring prophylactic treatment.
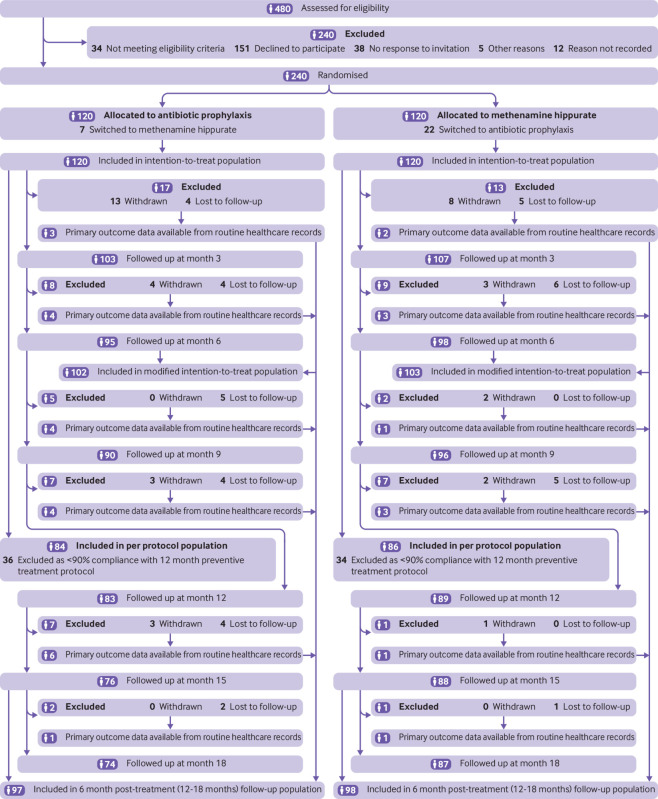
Interventions: Random assignment (1:1, using permuted blocks of variable length via a web based system) to receive antibiotic prophylaxis or methenamine hippurate for 12 months. Treatment allocation was not masked and crossover between arms was allowed.
Main outcome measure: Absolute difference in incidence of symptomatic, antibiotic treated, urinary tract infections during treatment. A patient and public involvement group predefined the non-inferiority margin as one episode of urinary tract infection per person year. Analyses performed in a modified intention-to-treat population comprised all participants observed for at least six months.
Results: Participants were randomly assigned to antibiotic prophylaxis (n=120) or methenamine hippurate (n=120). The modified intention-to-treat analysis comprised 205 (85%) participants (antibiotics, n=102 (85%); methenamine hippurate, n=103 (86%)). Incidence of antibiotic treated urinary tract infections during the 12 month treatment period was 0.89 episodes per person year (95% confidence interval 0.65 to 1.12) in the antibiotics group and 1.38 (1.05 to 1.72) in the methenamine hippurate group, with an absolute difference of 0.49 (90% confidence interval 0.15 to 0.84) confirming non-inferiority. Adverse reactions were reported by 34/142 (24%) in the antibiotic group and 35/127 (28%) in the methenamine group and most reactions were mild.
Conclusion: Non-antibiotic prophylactic treatment with methenamine hippurate might be appropriate for women with a history of recurrent episodes of urinary tract infections, informed by patient preferences and antibiotic stewardship initiatives, given the demonstration of non-inferiority to daily antibiotic prophylaxis seen in this trial.
Trial registration: ISRCTN70219762.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the NIHR HTA programme for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
ALTAR trial of antibiotic alternative in recurrent urinary infection is a step towards a more collective conversation.BMJ. 2022 Apr 12;377:o914. doi: 10.1136/bmj.o914. BMJ. 2022. PMID: 35414605 No abstract available.
-
Infection and Inflammation of the Genitourinary Tract.J Urol. 2022 Oct;208(4):912-913. doi: 10.1097/JU.0000000000002867. Epub 2022 Jul 28. J Urol. 2022. PMID: 35900131 No abstract available.
References
-
- National Institute for Health and Care Excellence. Guideline NG112, Urinary tract infection (recurrent): antimicrobial prescribing 2018. https://www.nice.org.uk/guidance/ng112/resources/urinary-tract-infection...
-
- European Association of Urology. EAU Guidelines – Urological Infections. Edn. presented at the EAU Annual Congress, Amsterdam, the Netherlands 2020. ISBN 978-94-92671-07-3.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical