

Autoantibodies targeting GPCRs and RAS-related molecules associate with COVID-19 severity
- PMID: 35264564
- PMCID: PMC8907309
- DOI: 10.1038/s41467-022-28905-5
Autoantibodies targeting GPCRs and RAS-related molecules associate with COVID-19 severity
Abstract
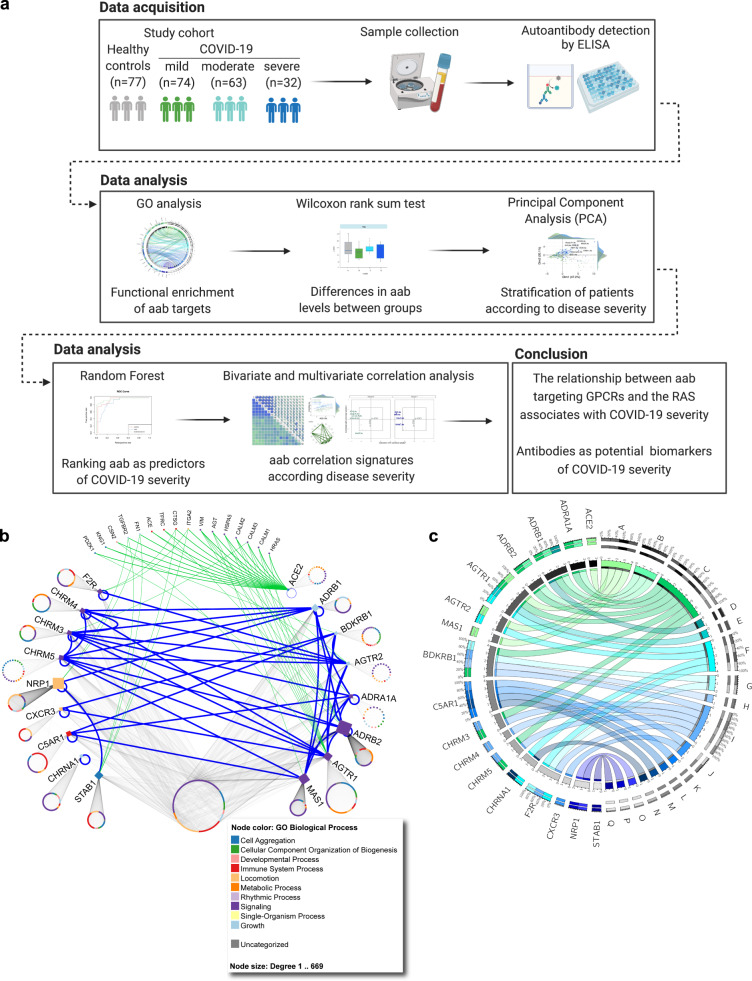
COVID-19 shares the feature of autoantibody production with systemic autoimmune diseases. In order to understand the role of these immune globulins in the pathogenesis of the disease, it is important to explore the autoantibody spectra. Here we show, by a cross-sectional study of 246 individuals, that autoantibodies targeting G protein-coupled receptors (GPCR) and RAS-related molecules associate with the clinical severity of COVID-19. Patients with moderate and severe disease are characterized by higher autoantibody levels than healthy controls and those with mild COVID-19 disease. Among the anti-GPCR autoantibodies, machine learning classification identifies the chemokine receptor CXCR3 and the RAS-related molecule AGTR1 as targets for antibodies with the strongest association to disease severity. Besides antibody levels, autoantibody network signatures are also changing in patients with intermediate or high disease severity. Although our current and previous studies identify anti-GPCR antibodies as natural components of human biology, their production is deregulated in COVID-19 and their level and pattern alterations might predict COVID-19 disease severity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that H.H. and K.S.F. are CellTrend managing directors and that GR is an advisor of CellTrend and earned an honorarium for her advice between 2011 and 2015. The other authors declare no competing interests.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
