

Impact of urban structure on infectious disease spreading
- PMID: 35264587
- PMCID: PMC8907266
- DOI: 10.1038/s41598-022-06720-8
Impact of urban structure on infectious disease spreading
Abstract
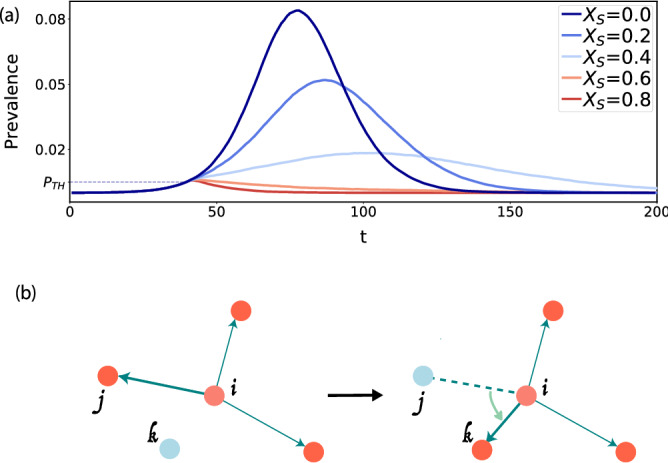
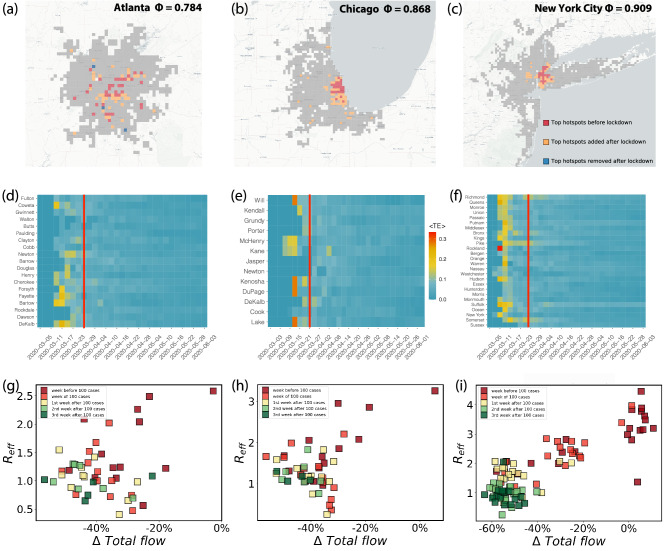
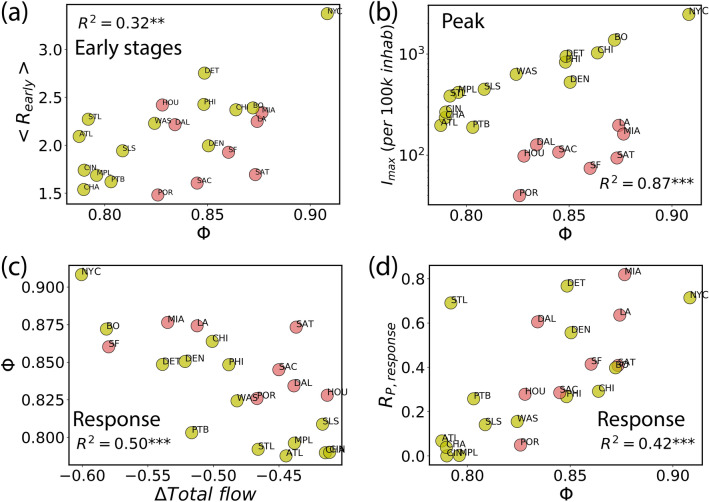
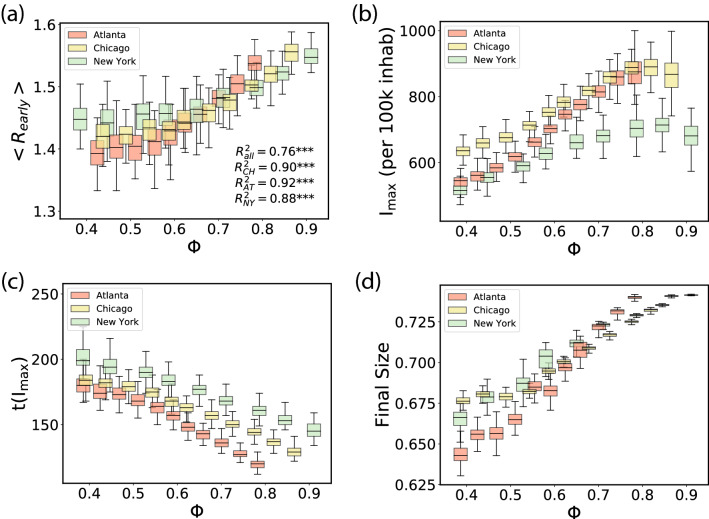
The ongoing SARS-CoV-2 pandemic has been holding the world hostage for several years now. Mobility is key to viral spreading and its restriction is the main non-pharmaceutical interventions to fight the virus expansion. Previous works have shown a connection between the structural organization of cities and the movement patterns of their residents. This puts urban centers in the focus of epidemic surveillance and interventions. Here we show that the organization of urban flows has a tremendous impact on disease spreading and on the amenability of different mitigation strategies. By studying anonymous and aggregated intra-urban flows in a variety of cities in the United States and other countries, and a combination of empirical analysis and analytical methods, we demonstrate that the response of cities to epidemic spreading can be roughly classified in two major types according to the overall organization of those flows. Hierarchical cities, where flows are concentrated primarily between mobility hotspots, are particularly vulnerable to the rapid spread of epidemics. Nevertheless, mobility restrictions in such types of cities are very effective in mitigating the spread of a virus. Conversely, in sprawled cities which present many centers of activity, the spread of an epidemic is much slower, but the response to mobility restrictions is much weaker and less effective. Investing resources on early monitoring and prompt ad-hoc interventions in more vulnerable cities may prove helpful in containing and reducing the impact of future pandemics.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Haug N, et al. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020;4:1303–1312. - PubMed
Publication types
MeSH terms
Grants and funding
- CSIC-COVID-19-039/CSIC funded by a contribution of AENA
- CSIC-COVID-19-039/CSIC funded by a contribution of AENA
- CSIC-COVID-19-039/CSIC funded by a contribution of AENA
- CSIC-COVID-19-039/CSIC funded by a contribution of AENA
- RTI2018-093732-B-C22/Agencia Estatal de Investigación
- RTI2018-093732-B-C22/Agencia Estatal de Investigación
- RTI2018-093732-B-C22/Agencia Estatal de Investigación
- RTI2018-093732-B-C22/Agencia Estatal de Investigación
- EP/S027920/1/UK EPSRC
- EP/S027920/1/UK EPSRC
- IIS-2029095/National Science Foundation
- IIS-2029095/National Science Foundation
- IIS-2029095/National Science Foundation
- W911NF-18-1-0421/Army Research Office
- W911NF-18-1-0421/Army Research Office
- W911NF-18-1-0421/Army Research Office
- FPI/2090/2018/Government of the Balearic Islands and the European Social Fund
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
