

Pattern of predictive features of continued cannabis use in patients with recent-onset psychosis and clinical high-risk for psychosis
- PMID: 35264631
- PMCID: PMC8907166
- DOI: 10.1038/s41537-022-00218-y
Pattern of predictive features of continued cannabis use in patients with recent-onset psychosis and clinical high-risk for psychosis
Abstract
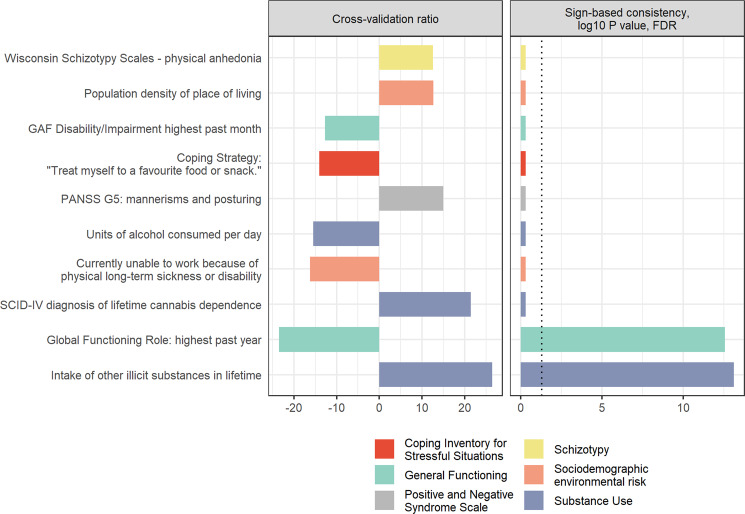
Continued cannabis use (CCu) is an important predictor for poor long-term outcomes in psychosis and clinically high-risk patients, but no generalizable model has hitherto been tested for its ability to predict CCu in these vulnerable patient groups. In the current study, we investigated how structured clinical and cognitive assessments and structural magnetic resonance imaging (sMRI) contributed to the prediction of CCu in a group of 109 patients with recent-onset psychosis (ROP). We tested the generalizability of our predictors in 73 patients at clinical high-risk for psychosis (CHR). Here, CCu was defined as any cannabis consumption between baseline and 9-month follow-up, as assessed in structured interviews. All patients reported lifetime cannabis use at baseline. Data from clinical assessment alone correctly classified 73% (p < 0.001) of ROP and 59 % of CHR patients. The classifications of CCu based on sMRI and cognition were non-significant (ps > 0.093), and their addition to the interview-based predictor via stacking did not improve prediction significantly, either in the ROP or CHR groups (ps > 0.065). Lower functioning, specific substance use patterns, urbanicity and a lack of other coping strategies contributed reliably to the prediction of CCu and might thus represent important factors for guiding preventative efforts. Our results suggest that it may be possible to identify by clinical measures those psychosis-spectrum patients at high risk for CCu, potentially allowing to improve clinical care through targeted interventions. However, our model needs further testing in larger samples including more diverse clinical populations before being transferred into clinical practice.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bhattacharyya S, et al. Individualized prediction of 2-year risk of relapse as indexed by psychiatric hospitalization following psychosis onset: Model development in two first episode samples. Schizophr. Res. 2021;228:483–492. - PubMed
-
- Schoeler T, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study. Lancet Psychiatry. 2016;3:947–953. - PubMed
-
- Schoeler T, et al. Continued versus discontinued cannabis use in patients with psychosis: a systematic review and meta-analysis. Lancet Psychiatry. 2016;3:215–225. - PubMed
