

Thoracic Paravertebral Block Combined with General Anaesthesia or General Anaesthesia Alone for Thoracoscopic Lung Adenocarcinoma Surgery: A Retrospective Study
- PMID: 35264885
- PMCID: PMC8901418
- DOI: 10.2147/CMAR.S346285
Thoracic Paravertebral Block Combined with General Anaesthesia or General Anaesthesia Alone for Thoracoscopic Lung Adenocarcinoma Surgery: A Retrospective Study
Abstract
Purpose: To investigate the effects of ultrasound-guided thoracic paravertebral block combined with general anaesthesia or general anaesthesia alone for thoracoscopic lung adenocarcinoma surgery, and to provide new thoughts for improving the clinical outcomes.
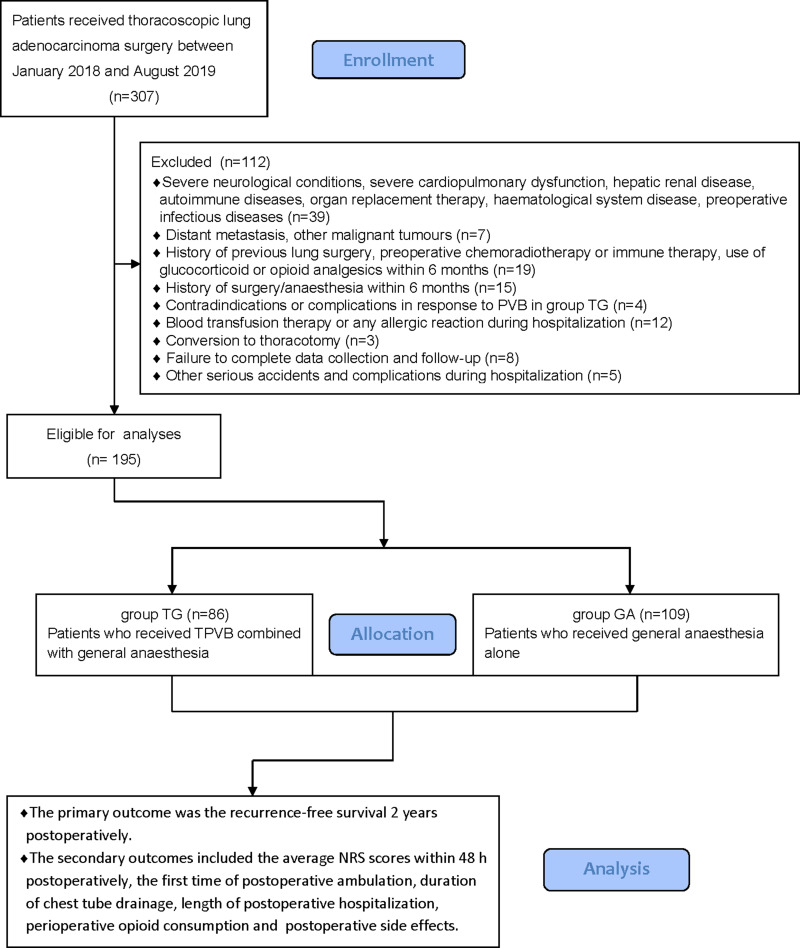
Methods: This was a retrospective study. Data were retrieved for 195 patients with lung adenocarcinoma undergoing elective radical lobectomy via video-assisted thoracoscopy between January 2018 and August 2019 in The Second Hospital of Shandong University, including 86 patients who received thoracic paravertebral block (TPVB) combined with general anaesthesia (group TG), and 109 patients who received general anaesthesia alone (group GA). All patients were given self-controlled intravenous analgesia pump for 48 h after surgery. The primary outcome was the recurrence-free survival 2 years postoperatively (the time between surgery and the earliest date of recurrence, metastasis or lung cancer-cause death). The secondary outcomes included the average numeric rating scale (NRS) scores within 48 h postoperatively, the first time of postoperative ambulation, duration of chest tube drainage, length of postoperative hospitalization, perioperative opioid consumption and the postoperative side effects.
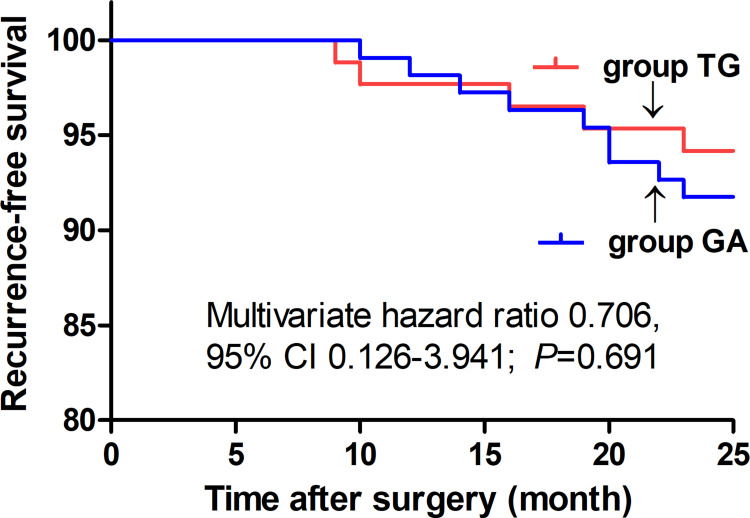
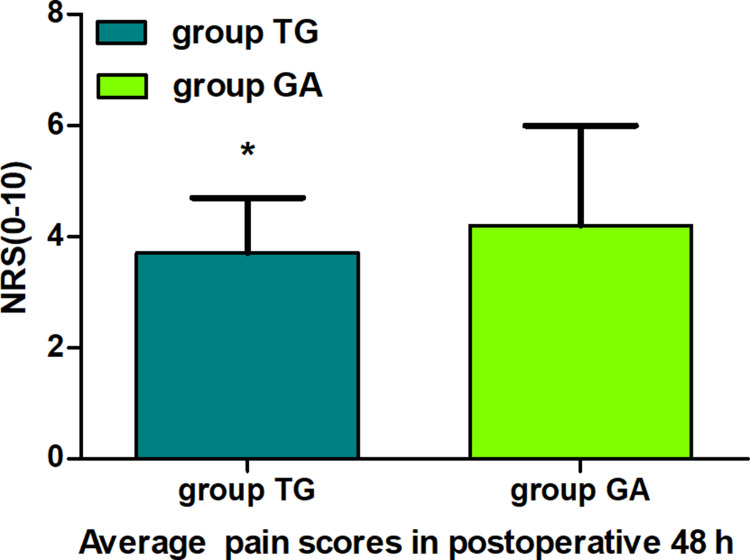
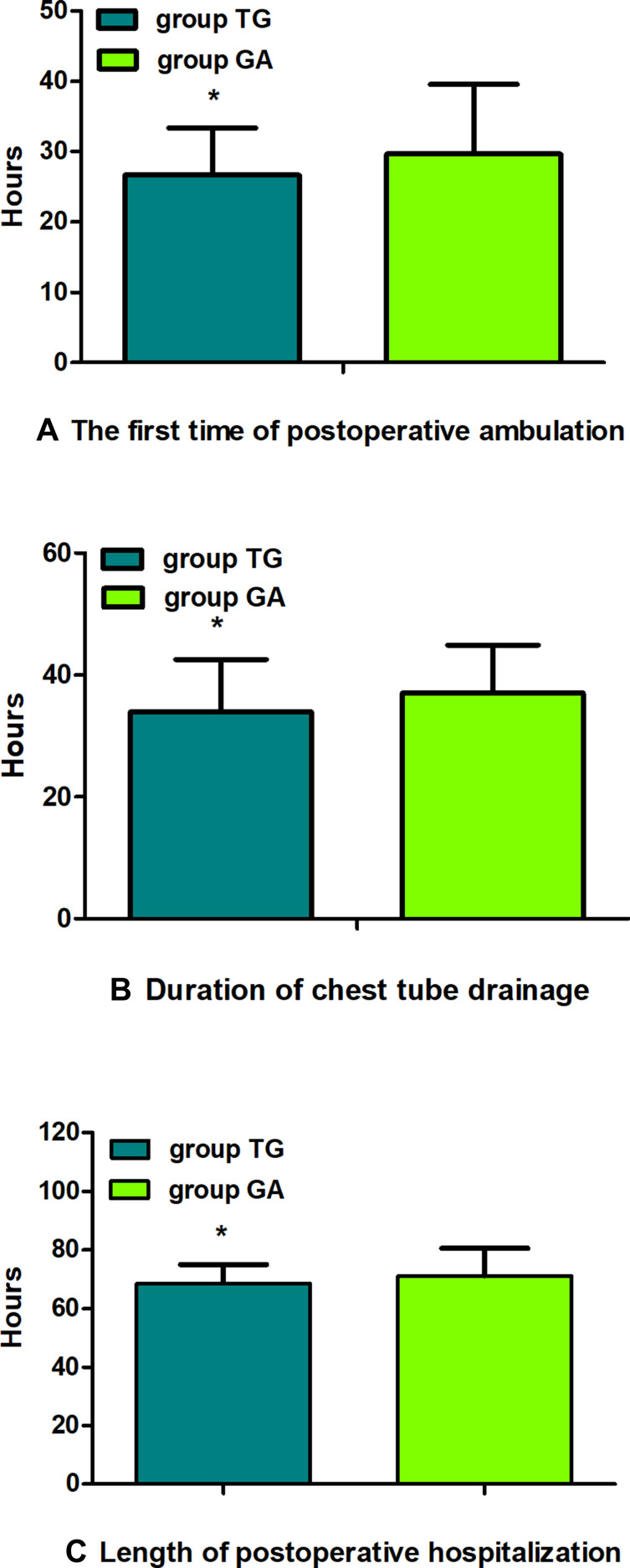
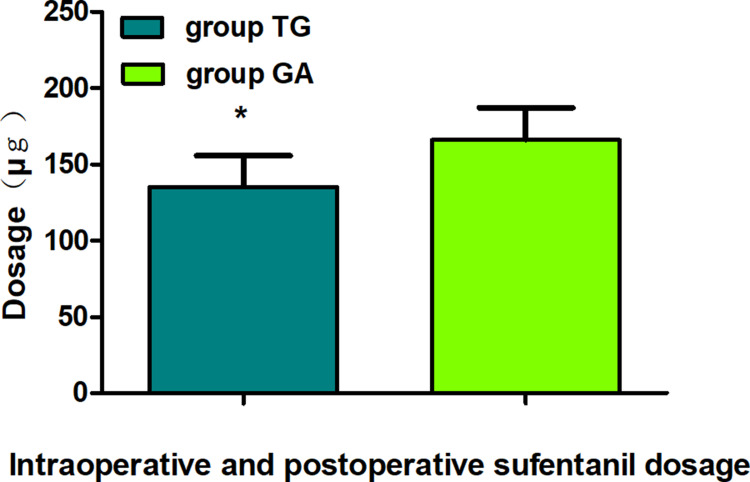
Results: There were no statistical differences in the recurrence-free survival 2 years postoperatively between groups (Multivariate hazard ratio 0.706, 95% CI 0.126-3.941, P=0.691). The average NRS scores within 48 h postoperatively were significantly lower in group TG (P<0.05). The first time of postoperative ambulation, duration of chest tube drainage, and length of postoperative hospitalization in group TG were significantly reduced (P<0.05). Opioid consumption was significantly decreased in group TG (P<0.01). Finally, the incidence of postoperative nausea and vomiting (PONV) was significantly lower in group TG (P<0.05).
Conclusion: TPVB for thoracoscopic lung adenocarcinoma surgery did not improve the recurrence-free survival 2 years postoperatively compared with general anaesthesia alone, but it significantly enhanced the postoperative analgesia effect, reduced opioid consumption as well as side effects, and accelerated postoperative early recovery.
Clinical trial registration number: The Chinese Clinical Trial Registry (ChiCTR-2100050454).
Keywords: lung adenocarcinoma; prognosis; thoracic paravertebral block; ultrasound guidance; video-assisted thoracoscopic surgery.
© 2022 Feng et al.
Conflict of interest statement
The authors declared no conflicts of interest for this work and no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Effect of oxycodone combined with ultrasound-guided thoracic paravertebral nerve block on postoperative analgesia in patients with lung cancer undergoing thoracoscopic surgery: protocol for a randomised controlled study.BMJ Open. 2023 Oct 16;13(10):e074416. doi: 10.1136/bmjopen-2023-074416. BMJ Open. 2023. PMID: 37844986 Free PMC article.
-
Effects of thoracic paravertebral block combined with s-ketamine on postoperative pain and cognitive function after thoracoscopic surgery.Heliyon. 2022 Dec 12;8(12):e12231. doi: 10.1016/j.heliyon.2022.e12231. eCollection 2022 Dec. Heliyon. 2022. PMID: 36578415 Free PMC article.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
-
Thoracic paravertebral block for perioperative lung preservation during VATS pulmonary surgery: study protocol of a randomized clinical trial.Trials. 2024 Jan 22;25(1):74. doi: 10.1186/s13063-023-07826-8. Trials. 2024. PMID: 38254233 Free PMC article.
-
Effect of thoracic paravertebral nerve block on delirium in patients after video-assisted thoracoscopic surgery: a systematic review and meta-analysis of randomized controlled trials.Front Neurol. 2024 Apr 10;15:1347991. doi: 10.3389/fneur.2024.1347991. eCollection 2024. Front Neurol. 2024. PMID: 38660094 Free PMC article.
Cited by
-
Ultrasound-Guided Quadratus Lumborum Block Combined with General Anaesthesia or General Anaesthesia Alone for Laparoscopic Radical Gastrectomy for Gastric Adenocarcinoma: A Monocentric Retrospective Study.Int J Gen Med. 2022 Oct 10;15:7739-7750. doi: 10.2147/IJGM.S382757. eCollection 2022. Int J Gen Med. 2022. PMID: 36249896 Free PMC article.
-
Anxiety evaluated by the Hospital Anxiety and Depression Scale as a predictor of postoperative nausea and vomiting: a pilot study.Nagoya J Med Sci. 2024 Feb;86(1):72-81. doi: 10.18999/nagjms.86.1.72. Nagoya J Med Sci. 2024. PMID: 38505720 Free PMC article.
-
Effects of Subcostal Anterior Quadratus Lumborum Block with and without Dexmedetomidine on Postoperative Rehabilitation in Patients Undergoing Laparoscopic Renal Surgery: A Prospective Double-Blinded Randomized Controlled Study.Drug Des Devel Ther. 2023 Nov 10;17:3281-3293. doi: 10.2147/DDDT.S422356. eCollection 2023. Drug Des Devel Ther. 2023. PMID: 38024533 Free PMC article. Clinical Trial.
-
Analgesic effect of thoracic paravertebral block on patients undergoing thoracoscopic lobectomy under general anesthesia.Pak J Med Sci. 2023 Nov-Dec;39(6):1774-1778. doi: 10.12669/pjms.39.6.7937. Pak J Med Sci. 2023. PMID: 37936771 Free PMC article.
-
Impact of thoracic paravertebral block and sufentanil on outcomes and postoperative cognitive dysfunction in thoracoscopic lung cancer surgery.World J Psychiatry. 2024 Jun 19;14(6):894-903. doi: 10.5498/wjp.v14.i6.894. eCollection 2024 Jun 19. World J Psychiatry. 2024. PMID: 38984344 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
