

Male Gender Is Associated with Lymph Node Metastasis but Not with Recurrence in Papillary Thyroid Carcinoma
- PMID: 35265124
- PMCID: PMC8901297
- DOI: 10.1155/2022/3534783
Male Gender Is Associated with Lymph Node Metastasis but Not with Recurrence in Papillary Thyroid Carcinoma
Abstract
Background: The incidence of papillary thyroid carcinoma (PTC) is higher in females than in males, but it remains unclear whether gender is associated with the aggressiveness of this disease. We aimed to clarify the influence of gender on the risk of developing lymph node metastasis (LNM) and on the prognosis of PTC patients. Study Design. Retrospective cohort study. Setting. Academic tertiary care center.
Methods: Clinical data of PTC patients who were admitted to the Department of Endocrine and Breast Surgery, the First Affiliated Hospital of Chongqing Medical University, between January 2013 and December 2018 were retrospectively reviewed. The differences in clinical features and outcomes between female and male patients were compared. Univariate and multivariate logistic regression analyses were conducted to assess the impact of gender on LNM. Kaplan-Meier curves were used to estimate recurrence-free survival (RFS).
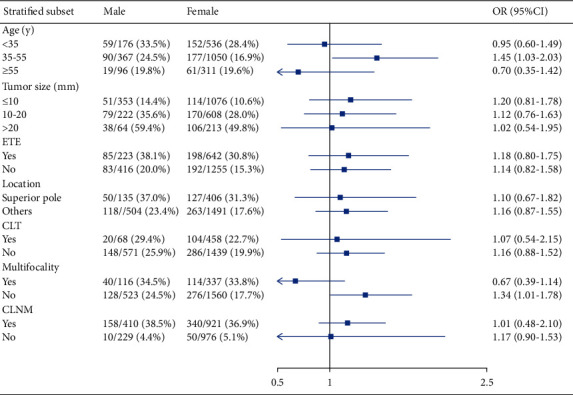
Results: A total of consecutive 2536 patients were enrolled in this study. Males accounted for 25.2% (639 cases) of all patients. Central lymph node metastasis (CLNM) and lateral lymph node metastasis (LLNM) rates were 52.5% (1346/2536) and 22.0% (558/2536), respectively. Male presented with higher LNM rates than female patients (65.7% vs. 51.2%; P < 0.001). Male gender was independently associated with LNM (OR = 1.93, 95% CI: 1.59-2.35; P < 0.001). After full adjustment, male gender still remained significantly associated with CLNM in all subgroups; however, subgroup analyses indicated no significant relationship between gender and LLNM. In addition, after a median follow-up period of 30 months, no significant difference was found in RFS between female and male patients (P=0.15).
Conclusions: This observational cohort study revealed that male gender was significantly associated with CLNM; whereas, LLNM was not different between female and male PTC patients in southwestern China. Moreover, currently, there is insufficient evidence to justify that male gender is an independent prognostic factor for recurrence.
Copyright © 2022 Jiang Zhu et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



Similar articles
-
Risk factors associated with lymph node metastasis in papillary thyroid cancer: a retrospective analysis based on 2,428 cases.Front Oncol. 2024 Nov 6;14:1473858. doi: 10.3389/fonc.2024.1473858. eCollection 2024. Front Oncol. 2024. PMID: 39568564 Free PMC article.
-
Predictive factors for central lymph node and lateral cervical lymph node metastases in papillary thyroid carcinoma.Clin Transl Oncol. 2019 Nov;21(11):1482-1491. doi: 10.1007/s12094-019-02076-0. Epub 2019 Mar 16. Clin Transl Oncol. 2019. PMID: 30879178
-
Clinical and pathologic predictors of lymph node metastasis in papillary thyroid microcarcinomas.Ann Diagn Pathol. 2020 Dec;49:151647. doi: 10.1016/j.anndiagpath.2020.151647. Epub 2020 Oct 22. Ann Diagn Pathol. 2020. PMID: 33126150
-
Influence of Obesity Parameters on Different Regional Patterns of Lymph Node Metastasis in Papillary Thyroid Cancer.Int J Endocrinol. 2022 Nov 7;2022:3797955. doi: 10.1155/2022/3797955. eCollection 2022. Int J Endocrinol. 2022. PMID: 36389127 Free PMC article.
-
A prediction model incorporating the BRAFV600E protein status for determining the risk of cervical lateral lymph node metastasis in papillary thyroid cancer patients with central lymph node metastasis.Eur J Surg Oncol. 2021 Nov;47(11):2774-2780. doi: 10.1016/j.ejso.2021.08.033. Epub 2021 Aug 27. Eur J Surg Oncol. 2021. PMID: 34483032
Cited by
-
Lymph Node Ratio Predicts Recurrence in Patients with Papillary Thyroid Carcinoma with Low Lymph Node Yield.Cancers (Basel). 2023 May 27;15(11):2947. doi: 10.3390/cancers15112947. Cancers (Basel). 2023. PMID: 37296909 Free PMC article.
-
Development and validation of a dynamic nomogram for predicting central lymph node metastasis in papillary thyroid carcinoma patients based on clinical and ultrasound features.Quant Imaging Med Surg. 2025 Feb 1;15(2):1555-1570. doi: 10.21037/qims-24-618. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995718 Free PMC article.
-
Gender differences in postoperative pain, sleep quality, and recovery outcomes in patients undergoing visual thoracoscopic surgery.Heliyon. 2024 Oct 5;10(19):e39015. doi: 10.1016/j.heliyon.2024.e39015. eCollection 2024 Oct 15. Heliyon. 2024. PMID: 39435074 Free PMC article.
-
Prediction of cervical lymph node metastasis in solitary papillary thyroid carcinoma based on ultrasound radiomics analysis.Front Oncol. 2024 Jan 25;14:1291767. doi: 10.3389/fonc.2024.1291767. eCollection 2024. Front Oncol. 2024. PMID: 38333681 Free PMC article.
-
Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter?Cancers (Basel). 2022 Apr 9;14(8):1896. doi: 10.3390/cancers14081896. Cancers (Basel). 2022. PMID: 35454803 Free PMC article.
References
LinkOut - more resources
Full Text Sources
