

Inadequate Bioavailability of Intramuscular Epinephrine in a Neonatal Asphyxia Model
- PMID: 35265564
- PMCID: PMC8899212
- DOI: 10.3389/fped.2022.828130
Inadequate Bioavailability of Intramuscular Epinephrine in a Neonatal Asphyxia Model
Abstract
Background: Over half a million newborn deaths are attributed to intrapartum related events annually, the majority of which occur in low resource settings. While progress has been made in reducing the burden of asphyxia, novel approaches may need to be considered to further decrease rates of newborn mortality. Administration of intravenous, intraosseous or endotracheal epinephrine is recommended by the Newborn Resuscitation Program (NRP) with sustained bradycardia at birth. However, delivery by these routes requires both advanced skills and specialized equipment. Intramuscular (IM) epinephrine may represent a simple, low cost and highly accessible alternative for consideration in the care of infants compromised at birth. At present, the bioavailability of IM epinephrine in asphyxia remains unclear.
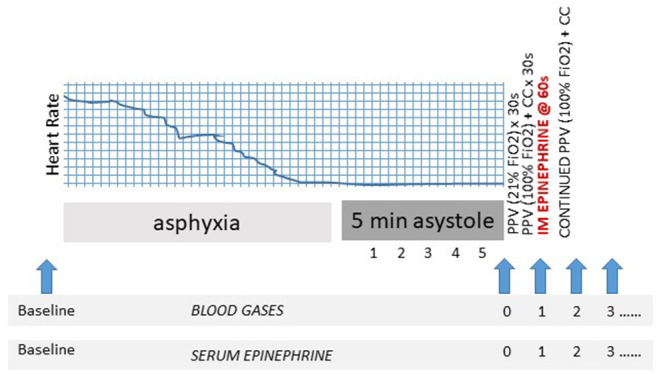
Methods: Four term fetal lambs were delivered by cesarean section and asphyxiated by umbilical cord occlusion with resuscitation after 5 min of asystole. IM epinephrine (0.1 mg/kg) was administered intradeltoid after 1 min of positive pressure ventilation with 30 s of chest compressions. Serial blood samples were obtained for determination of plasma epinephrine concentrations by ELISA.
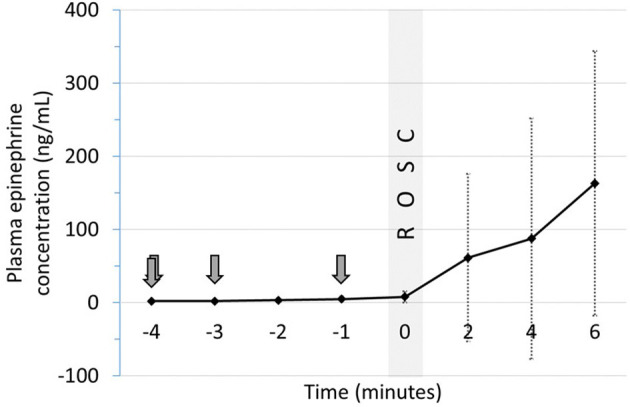
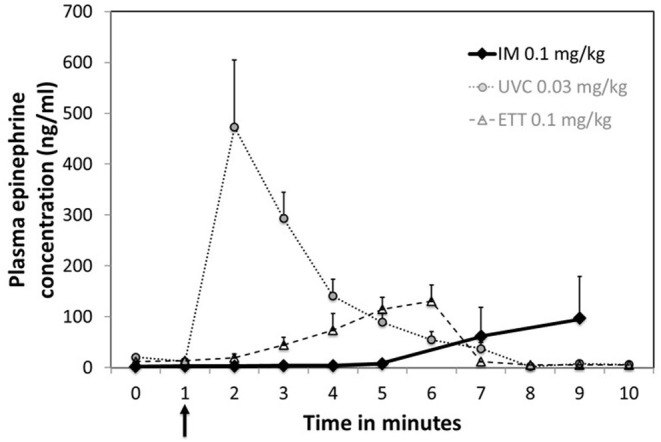
Results: Epinephrine concentrations failed to increase following administration via IM injection. Delayed absorption was observed after return of spontaneous circulation (ROSC) in half of the studies.
Conclusions: Inadequate absorption of epinephrine occurs with IM administration during asphyxial cardiac arrest, implying this route would be ineffective in infants who are severely compromised at birth. Late absorption following ROSC raises concerns for risks of side effects. However, the bioavailability and efficacy of intramuscular epinephrine in less profound asphyxia may warrant further evaluation.
Keywords: asphyxia; epinephrine; intramuscular; low-resource; neonatal; resuscitation.
Copyright © 2022 Berkelhamer, Vali, Nair, Gugino, Helman, Koenigsknecht, Nielsen and Lakshminrusimha.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer P-YC declared a past collaboration with one of the authors SL to the handling editor BN.
Figures
Similar articles
-
Comparison of intraosseous and intravenous epinephrine administration during resuscitation of asphyxiated newborn lambs.Arch Dis Child Fetal Neonatal Ed. 2022 May;107(3):311-316. doi: 10.1136/archdischild-2021-322638. Epub 2021 Aug 30. Arch Dis Child Fetal Neonatal Ed. 2022. PMID: 34462318
-
Evaluating the efficacy of endotracheal and intranasal epinephrine administration in severely asphyxic bradycardic newborn lambs: a randomised preclinical study.Arch Dis Child Fetal Neonatal Ed. 2025 Feb 21;110(2):207-212. doi: 10.1136/archdischild-2024-327348. Arch Dis Child Fetal Neonatal Ed. 2025. PMID: 39237256 Free PMC article.
-
Evaluation of Timing and Route of Epinephrine in a Neonatal Model of Asphyxial Arrest.J Am Heart Assoc. 2017 Feb 18;6(2):e004402. doi: 10.1161/JAHA.116.004402. J Am Heart Assoc. 2017. PMID: 28214793 Free PMC article.
-
Medications in neonatal resuscitation: epinephrine and the search for better alternative strategies.Clin Perinatol. 2012 Dec;39(4):843-55. doi: 10.1016/j.clp.2012.09.005. Clin Perinatol. 2012. PMID: 23164182 Review.
-
A Global View of Neonatal Asphyxia and Resuscitation.Front Pediatr. 2019 Nov 26;7:489. doi: 10.3389/fped.2019.00489. eCollection 2019. Front Pediatr. 2019. PMID: 31850287 Free PMC article. Review.
Cited by
-
Intramuscular versus intravenous epinephrine administration in a pediatric porcine model of cardiopulmonary resuscitation.Resusc Plus. 2024 Sep 13;20:100769. doi: 10.1016/j.resplu.2024.100769. eCollection 2024 Dec. Resusc Plus. 2024. PMID: 39309745 Free PMC article.
-
Femoral Occlusion during Neonatal Cardiopulmonary Resuscitation Improves Outcomes in an Ovine Model of Perinatal Cardiac Arrest.Children (Basel). 2023 Nov 13;10(11):1804. doi: 10.3390/children10111804. Children (Basel). 2023. PMID: 38002895 Free PMC article.
References
-
- UNICEF . Available online at: https://data.unicef.org/topic/child-survival/neonatal-mortality, (2019) (Accessed November 30, 2021).
-
- Department Department of Evidence Information Research Maternal Child Epidemiology Estimation (MCEE) . MCEE-WHO Methods and Data Sources for Child Causes of Death 2000-2016. Geneva: World Health Organization; (2018). Available online at: https://www.who.int/healthinfo/global_burden_disease/childcod_methods_20... (accessed November 30, 2021).
LinkOut - more resources
Full Text Sources
Miscellaneous