

Rare Genetic Variants Associated With Myocardial Fibrosis: Multi-Ethnic Study of Atherosclerosis
- PMID: 35265679
- PMCID: PMC8899004
- DOI: 10.3389/fcvm.2022.804788
Rare Genetic Variants Associated With Myocardial Fibrosis: Multi-Ethnic Study of Atherosclerosis
Abstract
Background: Rare pathogenic variants in cardiomyopathy (CM) genes can predispose to cardiac remodeling or fibrosis. We studied the carrier status for such variants in adults without clinical cardiovascular disease (CVD) in whom cardiac MRI (CMR)-derived measures of myocardial fibrosis were obtained in the Multi-Ethnic Study of Atherosclerosis (MESA).
Objectives: To identify CM-associated pathogenic variants and assess their relative prevalence in participants with extensive myocardial fibrosis by CMR.
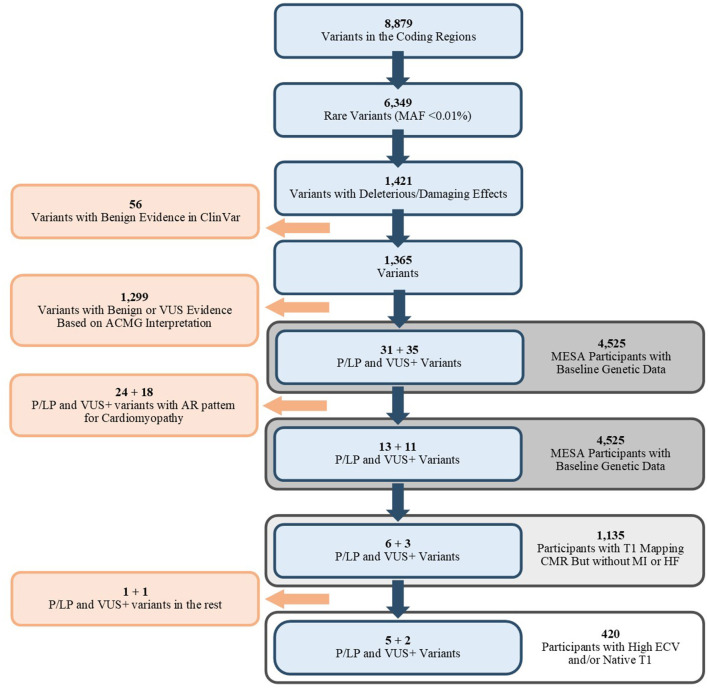
Methods: MESA whole-genome sequencing data was evaluated to capture variants in CM-associated genes (n = 82). Coding variants with a frequency of <0.1% in gnomAD and 1,000 Genomes Project databases and damaging/deleterious effects based on in-silico scoring tools were assessed by ClinVar database and ACMG curation guidelines for evidence of pathogenicity. Cases were participants with high myocardial fibrosis defined as highest quartile of extracellular volume (ECV) or native T1 time in T1-mapping CMR and controls were the remainder of participants.
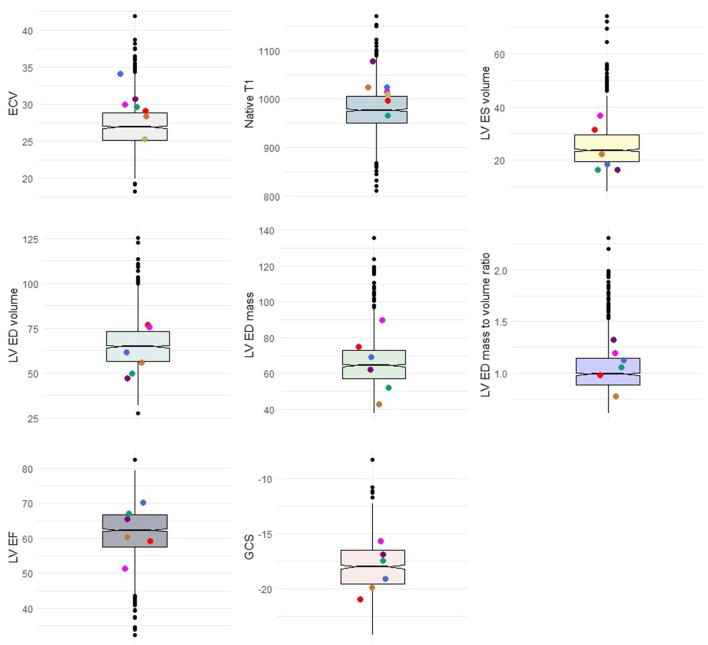
Results: A total of 1,135 MESA participants had available genetic data and phenotypic measures and were free of clinical CVD at the time of CMR. We identified 6,349 rare variants in CM-associated genes in the overall MESA population, of which six pathogenic/likely pathogenic (P/LP) variants were present in the phenotyped subpopulation. The genes harboring P/LP variants in the case group were MYH7, CRYAB, and SCN5A. The prevalence of P/LP rare variants in cases was higher than controls (5 in 420 [1.1%] vs. 1 in 715 [0.1%], p = 0.03). We identified two MYBPC3 Variants of Unknown Significance (VUS)s with borderline pathogenicity in the case group. The left ventricle (LV) volume, mass, ejection fraction (EF), and longitudinal and circumferential strain in participants with the variants were not different compared to the overall cohort.
Conclusions: We observed a higher prevalence of rare potentially pathogenic CM associated genetic variants in participants with significant myocardial fibrosis quantified in CMR as compared to controls without significant fibrosis. No cardiac structural or functional differences were found between participants with or without P/LP variants.
Keywords: T1; cardiomyopathy; fibrosis; genetics; interstitial; magnetic resonance imaging; rare.
Copyright © 2022 Shabani, Dutta, Ambale-Venkatesh, Post, Taylor, Rich, Wu, Pereira, Shah, Chatterjee, Rotter, Arking and Lima.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor declared a past co-authorship with one of the authors with the authors WP, KT, SR, JR, and JL.
Figures
References
-
- Venkatesh BA, Donekal S, Yoneyama K, Wu C, Fernandes VR, Rosen BD, et al. Regional myocardial functional patterns: quantitative tagged magnetic resonance imaging in an adult population free of cardiovascular risk factors: the multi-ethnic study of atherosclerosis (MESA). J Magn Reson Imaging. (2015) 42:153–9. 10.1002/jmri.24749 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous