

Risk Factors for and Clinical Outcomes of Polymicrobial Acinetobacter baumannii Bloodstream Infections
- PMID: 35265714
- PMCID: PMC8898812
- DOI: 10.1155/2022/5122085
Risk Factors for and Clinical Outcomes of Polymicrobial Acinetobacter baumannii Bloodstream Infections
Abstract
Background: Although the clinical features of Acinetobacter baumannii bloodstream infection are well described, the specific clinical characteristics of polymicrobial Acinetobacter baumannii bloodstream infection have been rarely reported. The objective of this study was to examine the risk factors for and clinical outcomes of polymicrobial Acinetobacter baumannii bloodstream infection.
Methods: A retrospective observational study was performed from January 2013 to December 2018 in a tertiary hospital. All patients with Acinetobacter baumannii bloodstream infection were enrolled, and the data were collected from the electronic medical records.
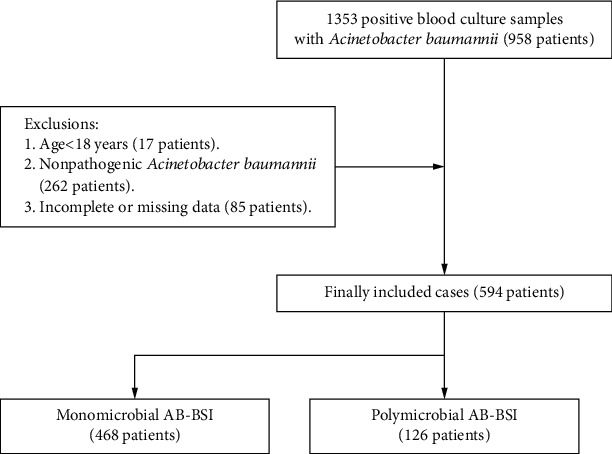
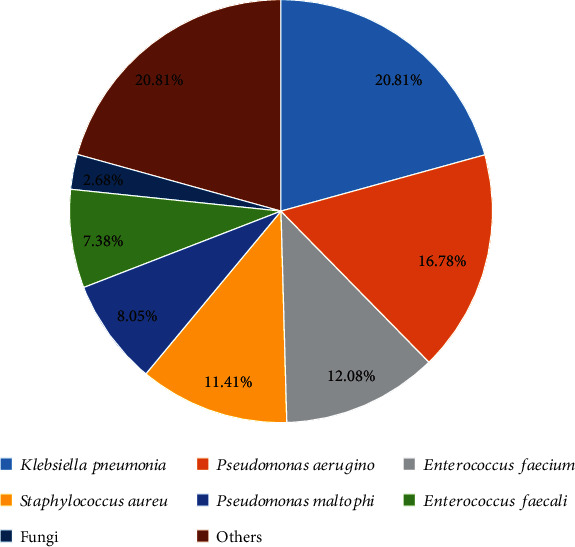
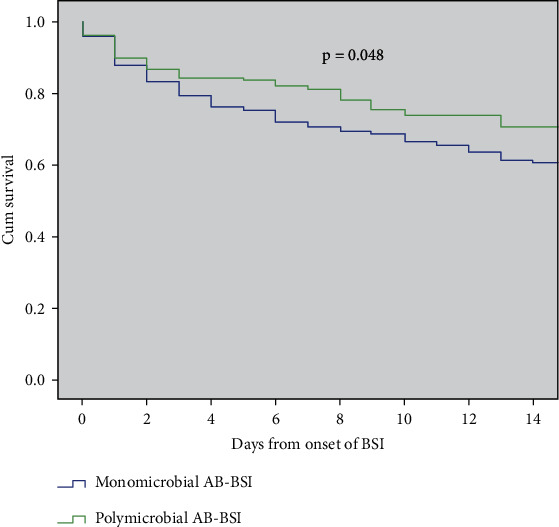
Results: A total of 594 patients were included, 21% (126/594) of whom had polymicrobial infection. The most common copathogen was Klebsiella pneumoniae (20.81%), followed by Pseudomonas aeruginosa (16.78%) and Enterococcus faecium (12.08%). Compared with monomicrobial Acinetobacter baumannii bloodstream infection, polymicrobial Acinetobacter baumannii bloodstream infection mostly originated from the skin and soft tissue (28.6% vs. 10.5%, p < 0.001). Multivariate analysis revealed that burn injury was independently associated with polymicrobial Acinetobacter baumannii bloodstream infection (adjusted odds ratio, 3.569; 95% confidence interval, 1.954-6.516). Patients with polymicrobial Acinetobacter baumannii bloodstream infection were more likely to have a longer hospital length of stay [40 (21, 68) vs. 27 (16, 45), p < 0.001] and more hospitalization days after bloodstream infection than those with monomicrobial Acinetobacter baumannii bloodstream infection [22 (8, 50) vs. 13 (4, 28), p < 0.001]. However, no significant difference in mortality was observed between the two groups.
Conclusions: Approximately one-fifth of Acinetobacter baumannii bloodstream infections were polymicrobial in this cohort. The main sources were skin and soft tissue infections, and burn injury was the only independent risk factor. Although mortality did not differ between the groups, considering the limitations of the study, further studies are required to assess the impact of polymicrobial (vs. monomicrobial) Acinetobacter baumannii bloodstream infection on outcomes.
Copyright © 2022 Zhenhua Qian et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest in this work.
Figures
References
-
- Fengcai S., Di X., Qianpeng H., Hongke Z., Yiyu D. Microbial characteristics in culture-positive sepsis and risk factors of polymicrobial infection in ICU. Zhonghua wei Zhong Bing ji jiu yi xue . 2015;27:718–723. - PubMed
-
- Kiratisin P., Chongthaleong A., Tan T. Y., et al. Comparative in vitro activity of carbapenems against major gram-negative pathogens: results of Asia-Pacific surveillance from the COMPACT II study. International Journal of Antimicrobial Agents . 2012;39:311–316. doi: 10.1016/j.ijantimicag.2012.01.002. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
