

Why digital health trials can fail: Lessons learned from a randomized trial of health coaching and virtual cardiac rehabilitation
- PMID: 35265897
- PMCID: PMC8890340
- DOI: 10.1016/j.cvdhj.2021.01.003
Why digital health trials can fail: Lessons learned from a randomized trial of health coaching and virtual cardiac rehabilitation
Abstract
Background: We performed a trial to evaluate the efficacy of a blended intervention with personalized health coaching and virtual cardiac rehabilitation to improve medication adherence and risk factors. The trial was terminated early. Here, we describe findings from a root cause analysis and lessons learned.
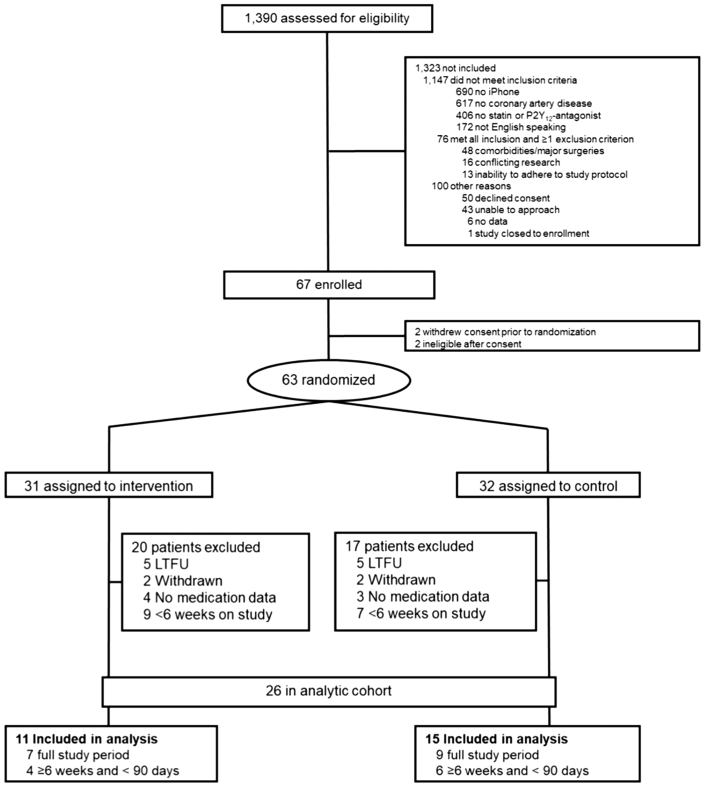
Methods: SmartGUIDE was an open-label, single-center trial that randomized participants with coronary artery disease who were prescribed a statin and/or P2Y12 inhibitor 1:1 to either usual care or the added use of a mobile app with components of cardiac rehabilitation paired with personal virtual coaching. The primary outcome was medication adherence: proportion of days covered (PDC). The planned sample size was 132. We performed a root cause analysis to evaluate processes from study development to closure.
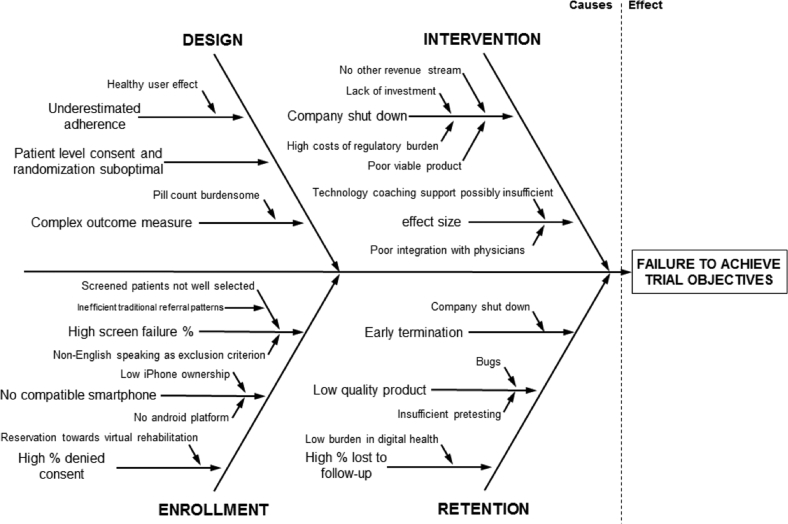
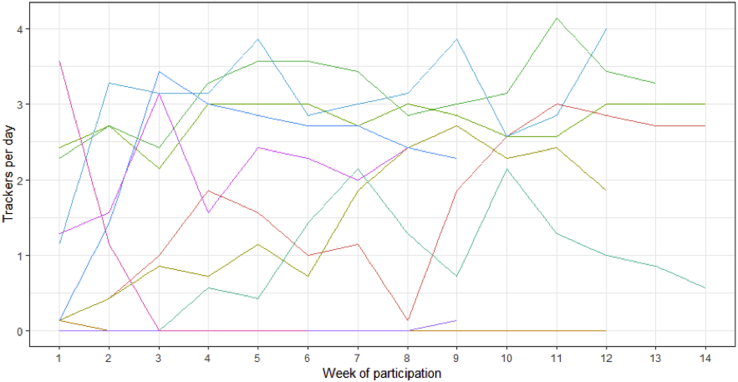
Results: During trial conduct, the technology start-up withdrew the intervention. The study was terminated early with 63 participants randomized and data from 26 available for analysis. The median PDC was high in both groups (intervention group 94%, interquartile range [IQR] 88%-96%; control group: 99%, IQR 95%-100%). Root cause analysis identified factors for not achieving trial objectives: key factors that limited enrollment (inclusion criteria, low penetration of compatible smartphones), participant retention or engagement (poor app product, insufficient technology support), and suboptimal choice of a technology partner (technology start-up's inexperience in health care, poor product design, inadequate fundraising).
Conclusion: We identified important and preventable factors leading to trial failure. These factors may be common across digital health trials and may explain prior observations that many such trials are never completed. Careful vetting of technology partners and more pragmatic study designs may prevent these missteps.
Keywords: Adherence; Cardiovascular risk factor; Coronary artery disease; Digital health; Digital platform; Mobile health; mHealth.
Figures
References
-
- Kurlansky P., Herbert M., Prince S., Mack M. Coronary artery bypass graft versus percutaneous coronary intervention clinical perspective. Circulation. 2016;134:1238–1246. - PubMed
-
- Ho P.M., Spertus J.A., Masoudi F.A., et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med. 2006;166:1842–1847. - PubMed
-
- Anglada-Martinez H., Riu-Viladoms G., Martin-Conde M., Rovira-Illamola M., Sotoca-Momblona J.M., Codina-Jane C. Does mHealth increase adherence to medication? Results of a systematic review. Int J Clin Pract. 2015;69:9–32. - PubMed
-
- Thakkar J., Kurup R., Laba T.-L., et al. Mobile telephone text messaging for medication adherence in chronic disease: a meta-analysis. JAMA Intern Med. 2016;176:340–349. - PubMed
-
- Shore S., Ho P.M., Lambert-Kerzner A., et al. Site-level variation in and practices associated with dabigatran adherence. JAMA. 2015;313:1443–1450. - PubMed
LinkOut - more resources
Full Text Sources
