

Electrical management of heart failure: from pathophysiology to treatment
- PMID: 35265992
- PMCID: PMC9123241
- DOI: 10.1093/eurheartj/ehac088
Electrical management of heart failure: from pathophysiology to treatment
Abstract
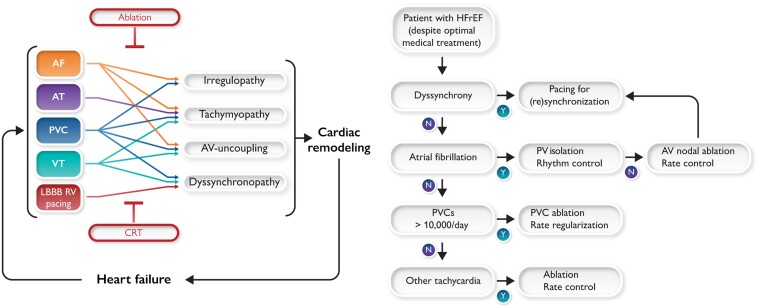
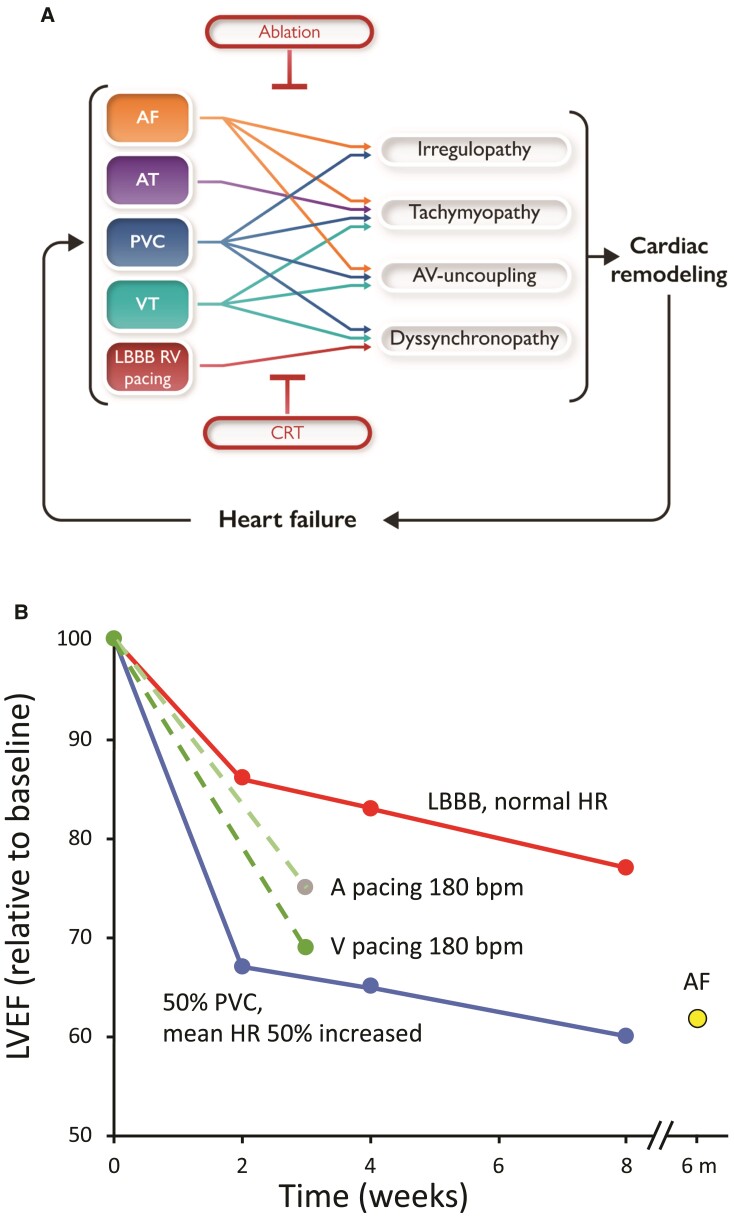
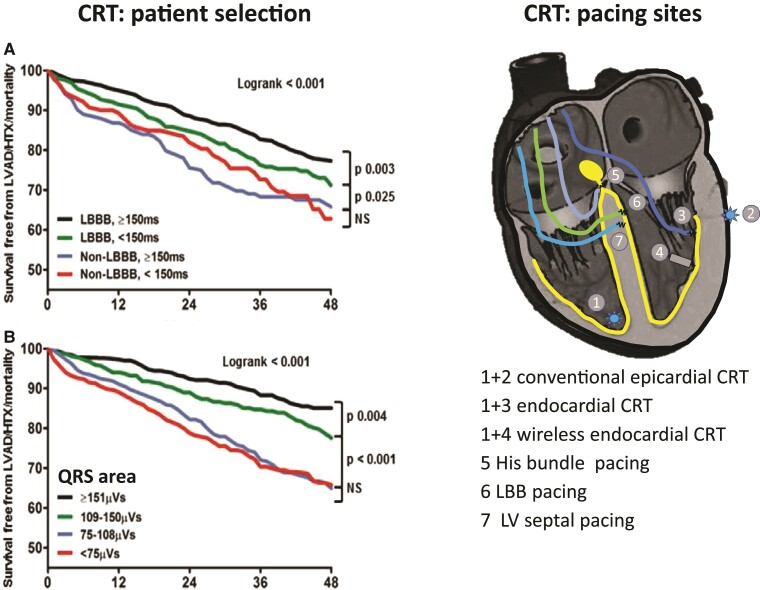
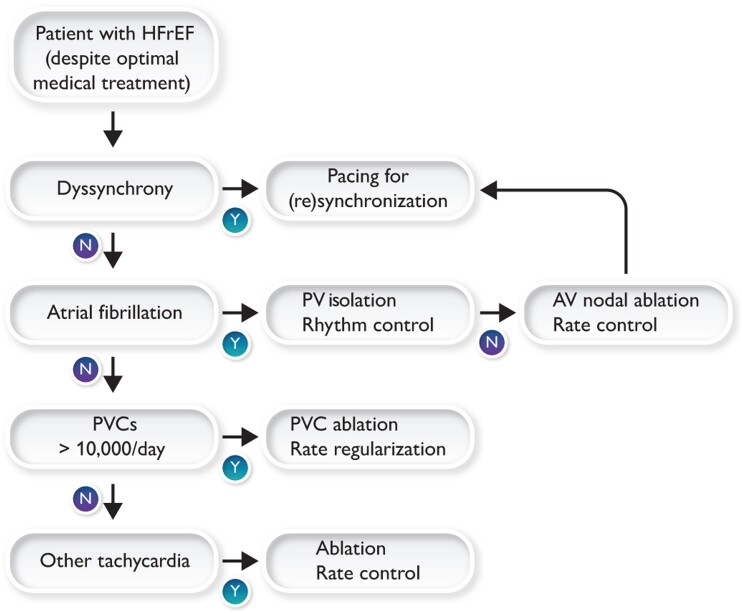
Electrical disturbances, such as atrial fibrillation (AF), dyssynchrony, tachycardia, and premature ventricular contractions (PVCs), are present in most patients with heart failure (HF). While these disturbances may be the consequence of HF, increasing evidence suggests that they may also cause or aggravate HF. Animal studies show that longer-lasting left bundle branch block, tachycardia, AF, and PVCs lead to functional derangements at the organ, cellular, and molecular level. Conversely, electrical treatment may reverse or mitigate HF. Clinical studies have shown the superiority of atrial and pulmonary vein ablation for rhythm control and AV nodal ablation for rate control in AF patients when compared with medical treatment. Ablation of PVCs can also improve left ventricular function. Cardiac resynchronization therapy (CRT) is an established adjunct therapy currently undergoing several interesting innovations. The current guideline recommendations reflect the safety and efficacy of these ablation therapies and CRT, but currently, these therapies are heavily underutilized. This review focuses on the electrical treatment of HF with reduced ejection fraction (HFrEF). We believe that the team of specialists treating an HF patient should incorporate an electrophysiologist in order to achieve a more widespread use of electrical therapies in the management of HFrEF and should also include individual conditions of the patient, such as body size and gender in therapy fine-tuning.
Keywords: ablation; atrial fibrillation; heart failure; premature ventricular contractions; resynchronization therapy; tachycardia; ventricular dyssynchrony.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
References
-
- Dickstein K, Normann C, Auricchio A, Bogale N, Cleland JG, Gitt AK, et al. CRT Survey II: an ESC survey of cardiac resynchronization therapy in 11088 patients—who is doing what to whom and how? Eur J Heart Fail 2018;20:1039–1051. - PubMed
-
- Lund LH, Benson L, Ståhlberg M, Braunschweig F, Edner M, Dahlström U, et al. Age, prognostic impact of QRS prolongation and left bundle branch block, and utilization of cardiac resynchronization therapy: findings from 14 713 patients in the Swedish Heart Failure Registry. Eur J Heart Fail 2014;16:1073–1081. - PubMed
-
- Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol 2003;91:2D–8D. - PubMed
-
- Vernooy K, Verbeek XA, Peschar M, Crijns HJGM, Arts T, Cornelussen RNM, et al. Left bundle branch block induces ventricular remodelling and functional septal hypoperfusion. Eur Heart J 2005;26:91–98. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
