

Does an Internal Joint Stabilizer and Standardized Protocol Prevent Recurrent Instability in Complex Persistent Elbow Instability?
- PMID: 35266916
- PMCID: PMC9191335
- DOI: 10.1097/CORR.0000000000002159
Does an Internal Joint Stabilizer and Standardized Protocol Prevent Recurrent Instability in Complex Persistent Elbow Instability?
Abstract
Background: The treatment of complex persistent elbow instability after trauma is challenging. Previous studies on treatments have reported varied surgical techniques, which makes it difficult to establish a therapeutic algorithm. Furthermore, the surgical procedures may not sufficiently restore elbow stability, even with an additional device, and a noted high rate of arthritis progression.While a recently developed internal joint stabilizer effectively treats elbow instability, its clinical application for complex persistent elbow instability is limited and the standardized protocol is not well described. Additionally, we want to know whether the arthritis progression will cause a negative impact on the functional outcomes of complex persistent elbow instability.
Questions/purposes: (1) Does treatment of complex persistent elbow instability with a hinged internal joint stabilizer and a standardized protocol prevent recurrent instability and other complications? (2) What are the pre- to postoperative improvements in pain, disability, elbow performance, and ROM? (3) Is the development of post-traumatic arthritis associated with worse pain, disability, elbow performance, and ROM?
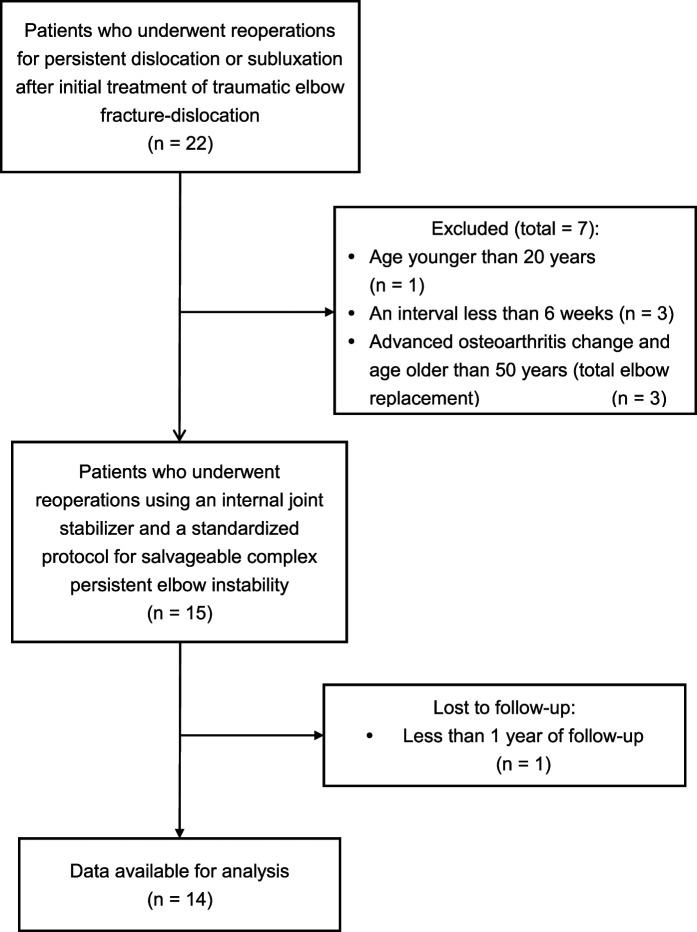
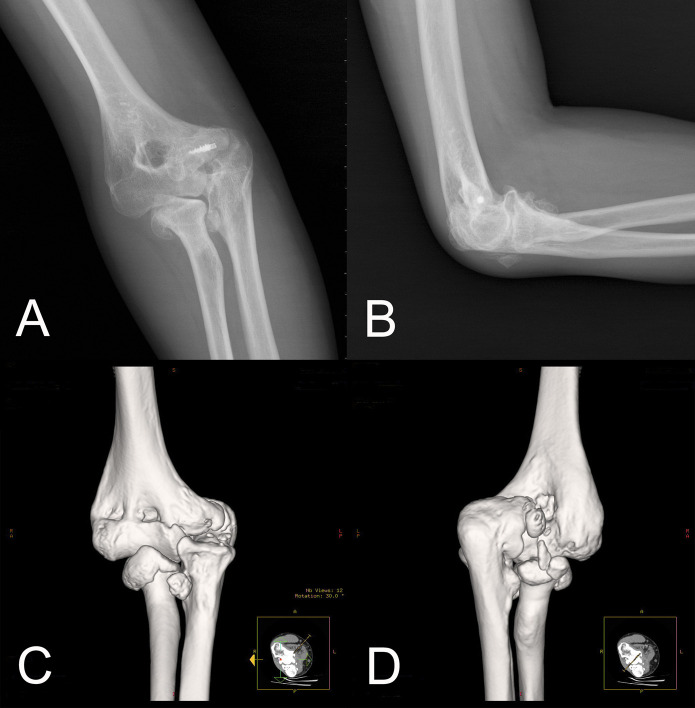
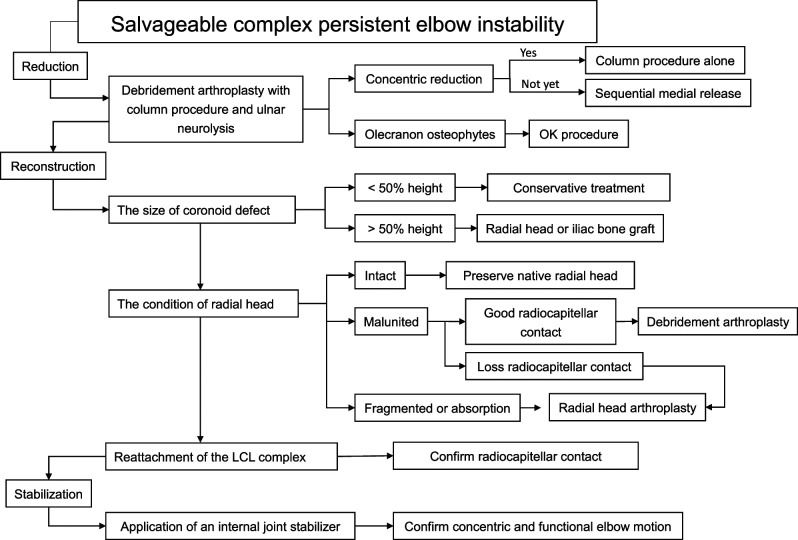
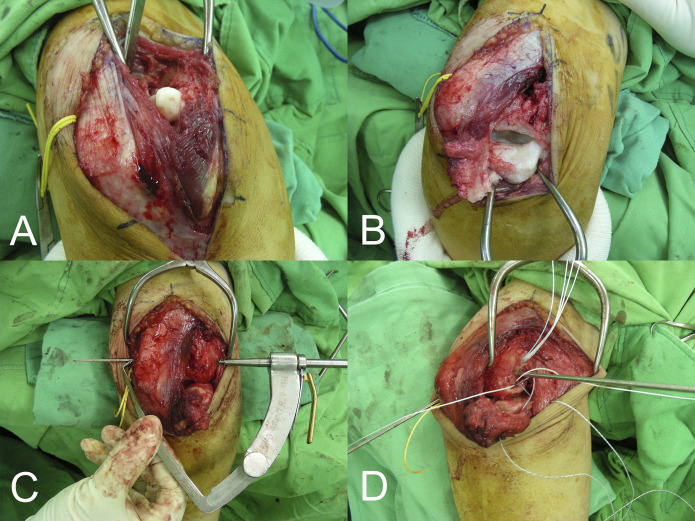
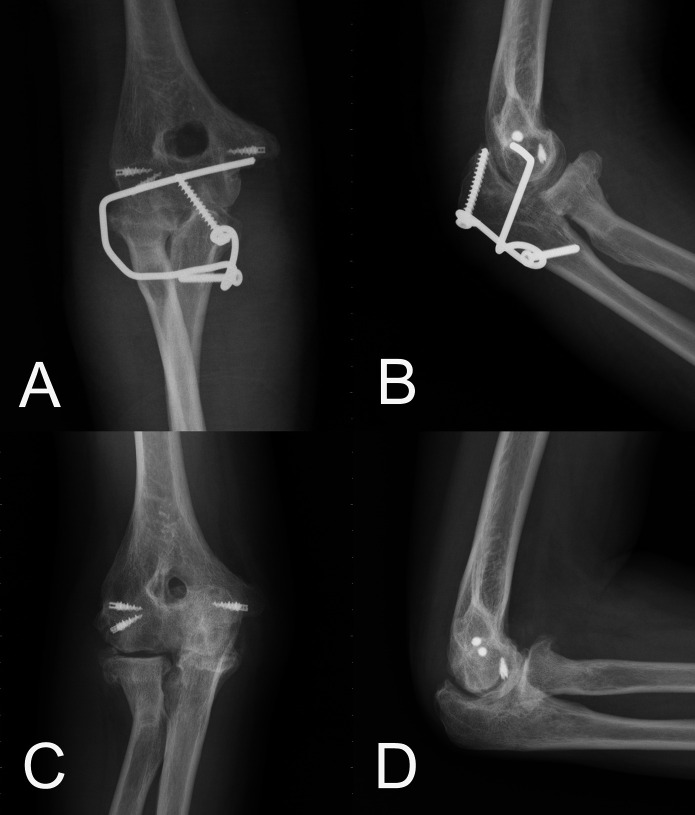
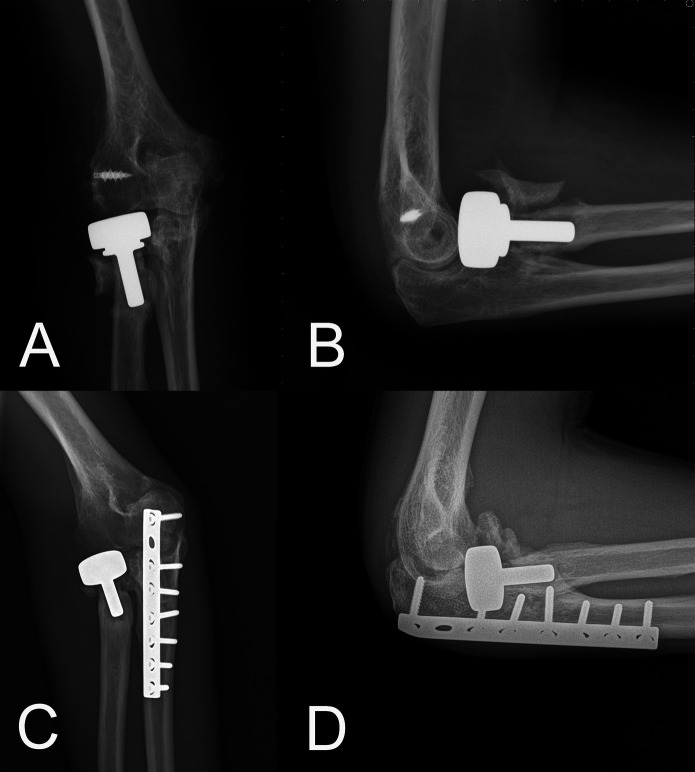
Methods: Between September 2014 and October 2019, we treated 22 patients for persistent dislocation or subluxation after initial treatment of traumatic elbow fracture-dislocations. Of those, we considered patients who were at least 20 years of age, with an interval of 6 weeks or more between the injury (initial treatment) and the index reconstructive procedure, which had been performed at our institute, as potentially eligible. During that time, we used an internal joint stabilizer with a standardized protocol for posttraumatic complex persistent elbow instability. We performed total elbow replacements in patients older than 50 years who had advanced elbow arthritis. Based on that, 82% (18 of 22) of patients were eligible; 14% (3 of 22) were excluded because total elbow replacements was undertaken, and another 5% (1 of 22) were lost before the minimum study follow-up of 1 year (median 24 months [range 12 to 63]), leaving 64% (14 of 22) for analysis in this retrospective study. We treated 14 patients (14 elbows) with posttraumatic complex persistent elbow instability with an internal joint stabilizer and a standardized protocol that comprised debridement arthroplasty with ulnar neurolysis, restoration of bony and ligamentous (reattachment) structures, application of an internal joint stabilizer, and early rehabilitation. There were eight men and six women in this study, with a median (range) age of 44 years (21 to 68). The initial elbow fracture-dislocation injury pattern was a terrible triad injury in seven patients, a posterolateral rotatory injury in four patients, and a posterior Monteggia fracture in three patients. Preoperative and follow-up radiographs were reviewed for evidence of recurrent instability and arthritis. Complications such as wound infection, seroma, neurovascular injury, and hardware complications were ascertained through chart review. Preoperative and postoperative VAS score for pain, DASH, and Mayo Elbow Performance Scores (MEPS) were collected and compared. Furthermore, extension-flexion and supination-pronation arcs were collected by chart review. We divided the patients into two groups according to whether or not they developed posttraumatic arthritis. We then presented the differences between pain, disability, elbow performance, and ROM. The hinged internal joint stabilizer was removed using another open procedure under general anesthesia 6 to 8 weeks after surgery.
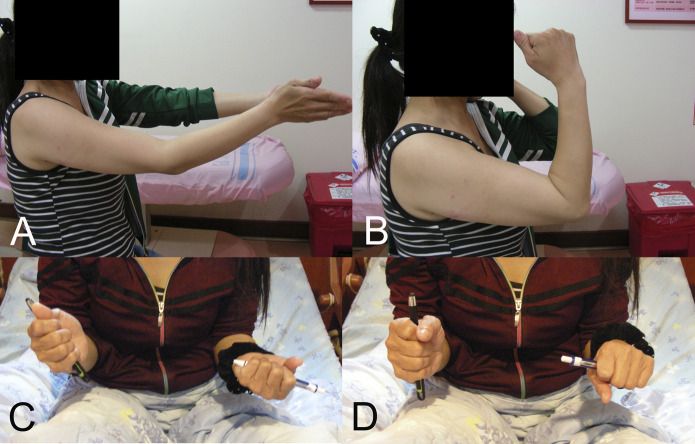
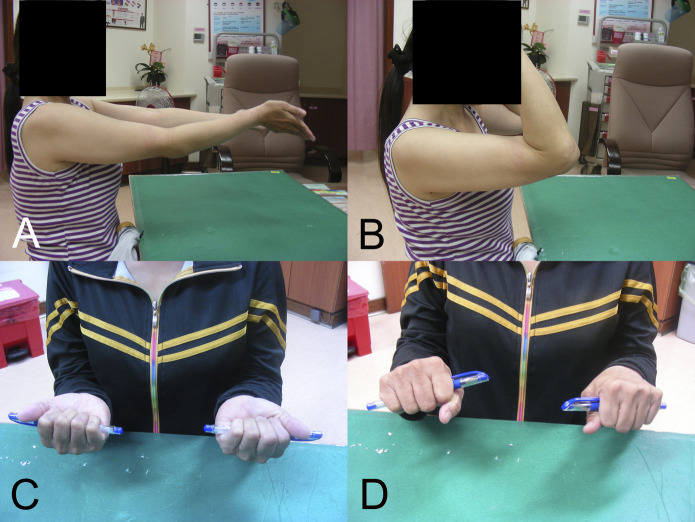
Results: There were no recurrent instability during and after device removal. Seven patients developed complications, including wound infection, seroma, neurovascular injury, hardware complications, and heterotopic ossification. Two patients had complications related to internal joint stabilizers and three had complications linked to radial head prostheses. Median (range) preoperative to postoperative changes included decreased pain (VAS 5 [2 to 9] to 0 [0 to 3], difference of medians -5; p < 0.001), decreased disability (DASH 41 [16 to 66] to 7 [0 to 46], difference of medians -34; p < 0.001), improved function (MEPS 60 [25 to 70] to 95 [65 to 100], difference of medians 35; p < 0.001), improved extension-flexion arc (40° [10° to 70°] to 113° [75° to 140°], difference of medians 73°; p < 0.001), and supination-pronation arc (78° [30° to 165°] to 148° [70° to 175°], difference of medians 70°; p < 0.001). Between patients with and without development of post-traumatic arthritis, there were no differences in postoperative pain (VAS 0 [0 to 3] to 0 [0 to 1], difference of medians 0; p = 0.17), disability (DASH 7 [0 to 46] to 7 [0 to 18], difference of medians 0; p = 0.40), function (MEPS 80 [65 to 100] to 95 [75 to 100], difference of medians 15; p = 0.79), extension-flexion arc (105° [75° to 140°] to 115° [80° to 125°], difference of medians 10°; p = 0.40), and supination-pronation arc (155° [125° to 175°] to 135° [70° to 160°], difference of medians -20°; p < 0.18).
Conclusion: In this small, retrospective study, we found that an internal joint stabilizer with a standardized treatment protocol could maintain concentric reduction while allowing early functional motion, and that it could improve clinical outcomes for patients with complex persistent elbow instability. However, patients must be counseled that the complications related to the radial head prostheses may occur, and that the benefits of early motion must compensate for an additional removal procedure and the risk of seroma formation.
Level of evidence: Level IV, therapeutic study.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no outside funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Similar articles
-
Single-staged treatment using a standardized protocol results in functional motion in the majority of patients with a terrible triad elbow injury.Clin Orthop Relat Res. 2014 Jul;472(7):2075-83. doi: 10.1007/s11999-014-3475-3. Clin Orthop Relat Res. 2014. PMID: 24474324 Free PMC article.
-
Terrible triad injuries of the elbow: does the coronoid always need to be fixed?Clin Orthop Relat Res. 2014 Jul;472(7):2084-91. doi: 10.1007/s11999-014-3471-7. Clin Orthop Relat Res. 2014. PMID: 24474322 Free PMC article.
-
Can we treat select terrible triad injuries nonoperatively?Clin Orthop Relat Res. 2014 Jul;472(7):2092-9. doi: 10.1007/s11999-014-3518-9. Clin Orthop Relat Res. 2014. PMID: 24549776 Free PMC article.
-
Chronic complex persistent elbow instability: a consecutive and prospective case series and review of recent literature.J Shoulder Elbow Surg. 2020 Apr;29(4):e103-e117. doi: 10.1016/j.jse.2019.11.021. J Shoulder Elbow Surg. 2020. PMID: 32197771 Review.
-
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique.J Bone Joint Surg Am. 2005 Mar;87 Suppl 1(Pt 1):22-32. doi: 10.2106/JBJS.D.02933. J Bone Joint Surg Am. 2005. PMID: 15743844 Review.
Cited by
-
Internal brace augmentation in elbow varus posteromedial rotatory instability (VPMRI) allows early rehabilitation and prevents stiffness.Arch Orthop Trauma Surg. 2024 Dec 18;145(1):62. doi: 10.1007/s00402-024-05722-7. Arch Orthop Trauma Surg. 2024. PMID: 39694925
-
Internal joint stabilizer covered by an anconeus flap for elbow instability: surgical technique and preliminary results.JSES Rev Rep Tech. 2024 Apr 7;4(3):476-484. doi: 10.1016/j.xrrt.2024.03.008. eCollection 2024 Aug. JSES Rev Rep Tech. 2024. PMID: 39157257 Free PMC article. No abstract available.
-
Using External Joint Stabilizer - Elbow (EJS-E) for treating elbow instability-biomechanical assessment and clinical outcomes.BMC Musculoskelet Disord. 2022 Dec 29;23(1):1137. doi: 10.1186/s12891-022-06103-0. BMC Musculoskelet Disord. 2022. PMID: 36581852 Free PMC article.
-
Surgical revision after previous failed lateral ulnar collateral ligament (LUCL) reconstruction and persisting posterolateral rotatory instability (PLRI) of the Elbow: a retrospective multicentric analysis.Eur J Orthop Surg Traumatol. 2025 Mar 9;35(1):103. doi: 10.1007/s00590-025-04201-y. Eur J Orthop Surg Traumatol. 2025. PMID: 40057913
-
The safety of humeroradial fixation using Kirschner wires in children.Sci Rep. 2024 Dec 5;14(1):30317. doi: 10.1038/s41598-024-81397-9. Sci Rep. 2024. PMID: 39639069 Free PMC article.
References
-
- Arafiles RP. Neglected posterior dislocation of the elbow. A reconstruction operation. J Bone Joint Surg Br . 1987;69:199-202. - PubMed
-
- Brewley EE, Gorman RA, Christmas KN, Simon P, Chapel RJ, Mighell MA. Use of a modified Outerbridge-Kashiwagi procedure for the treatment of posttraumatic elbow sequelae. J Shoulder Elbow Surg . 2019;28:1387-1394. - PubMed
-
- Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg Am. 1986;68:669-674. - PubMed
-
- Chen NC, Jupiter JB, Steinmann SP, Ring D. Nonacute treatment of elbow fracture with persistent ulnohumeral dislocation or subluxation. J Bone Joint Surg Am . 2014;96:1308-1316. - PubMed
-
- Cheung EV, O’Driscoll SW, Morrey BF. Complications of hinged external fixators of the elbow. J Shoulder Elbow Surg . 2008;17:447-453. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
