

The Therapeutic Potential of FLASH-RT for Pancreatic Cancer
- PMID: 35267474
- PMCID: PMC8909276
- DOI: 10.3390/cancers14051167
The Therapeutic Potential of FLASH-RT for Pancreatic Cancer
Abstract
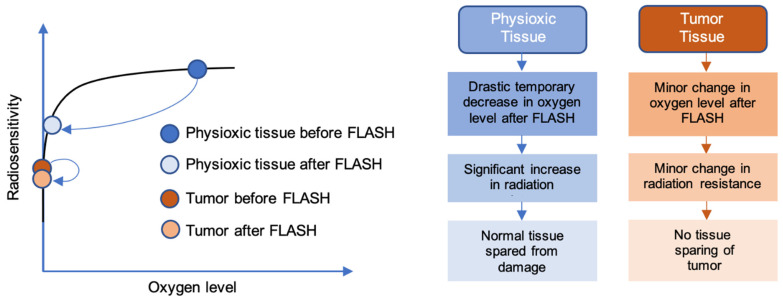
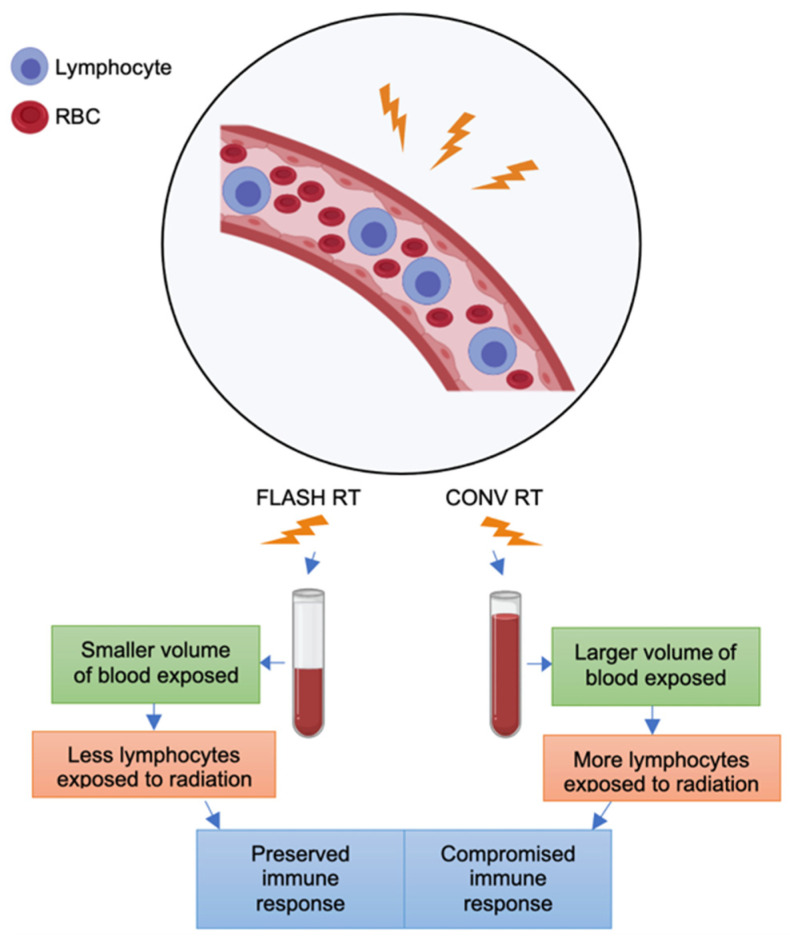
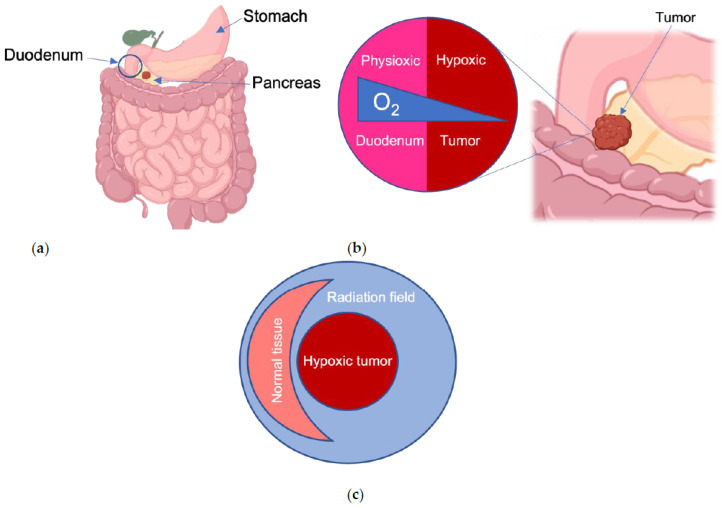
Recent preclinical evidence has shown that ionizing radiation given at an ultra-high dose rate (UHDR), also known as FLASH radiation therapy (FLASH-RT), can selectively reduce radiation injury to normal tissue while remaining isoeffective to conventional radiation therapy (CONV-RT) with respect to tumor killing. Unresectable pancreatic cancer is challenging to control without ablative doses of radiation, but this is difficult to achieve without significant gastrointestinal toxicity. In this review article, we explore the propsed mechanisms of FLASH-RT and its tissue-sparing effect, as well as its relevance and suitability for the treatment of pancreatic cancer. We also briefly discuss the challenges with regard to dosimetry, dose rate, and fractionation for using FLASH-RT to treat this disease.
Keywords: FLASH effect; FLASH radiation; conventional radiation; gastrointestinal toxicity; pancreatic cancer.
Conflict of interest statement
C.M.T. is on the medical advisory board of Accuray and is a paid consultant for Xerient Pharma and Phebra Pty, Ltd. E.S. and C.M.O. have no potential conflicts of interest.
Figures
References
-
- Thomas G.M. Concurrent chemotherapy and radiation for locally advanced cervical cancer: The new standard of care. Semin. Radiat. Oncol. 2000;10:44–50. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
