

Current Understanding of Hypoxia in Glioblastoma Multiforme and Its Response to Immunotherapy
- PMID: 35267480
- PMCID: PMC8909860
- DOI: 10.3390/cancers14051176
Current Understanding of Hypoxia in Glioblastoma Multiforme and Its Response to Immunotherapy
Abstract
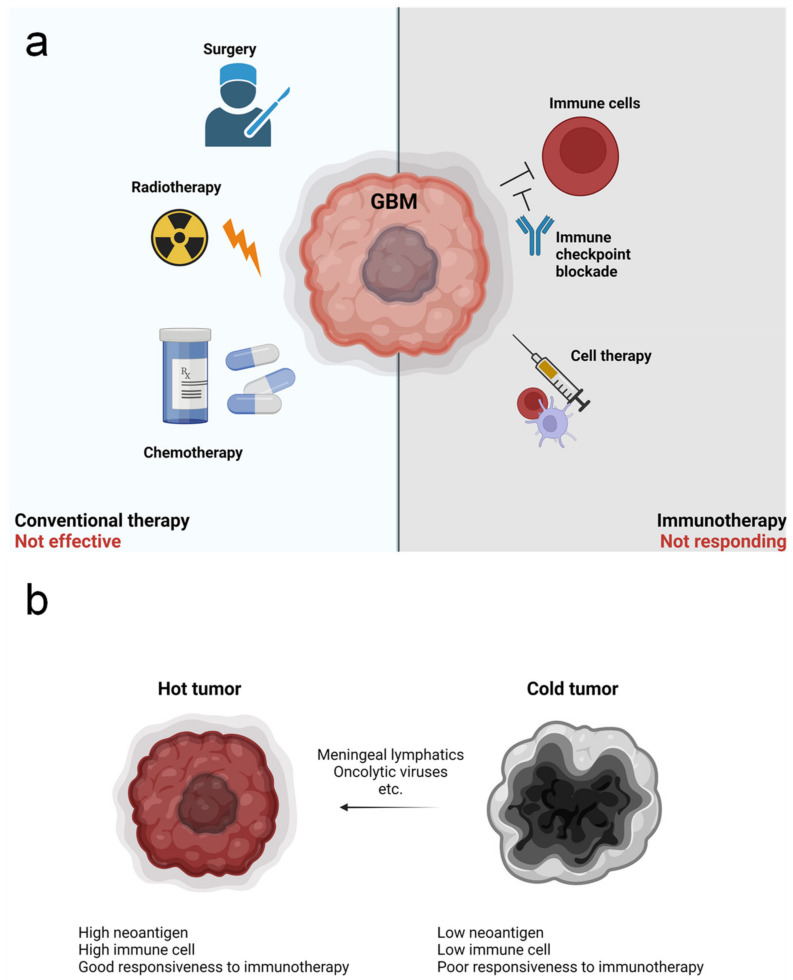
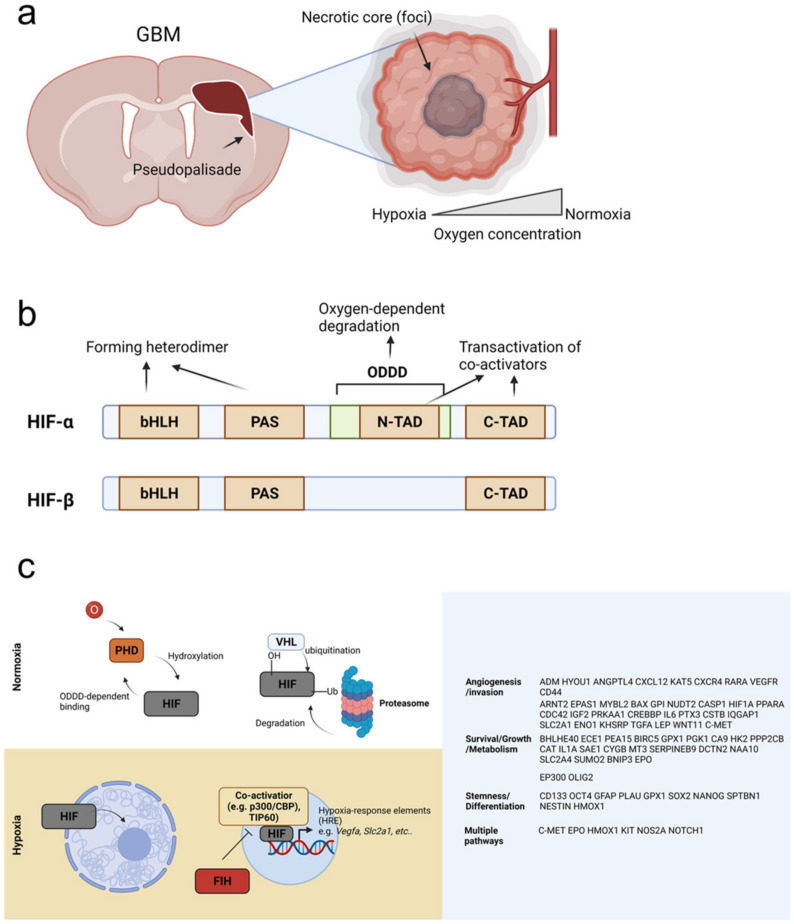
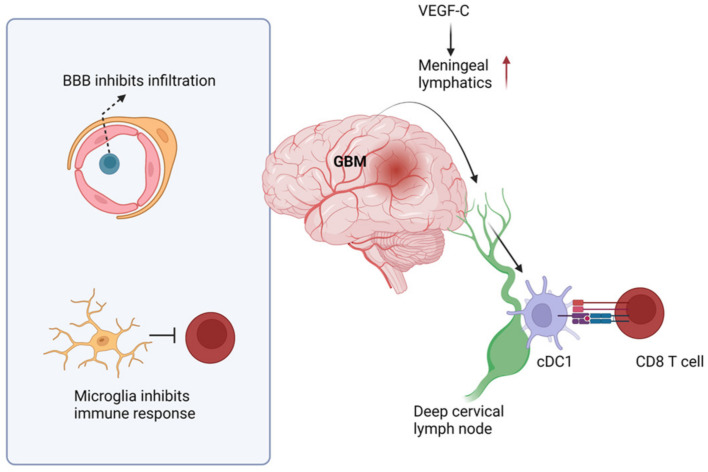
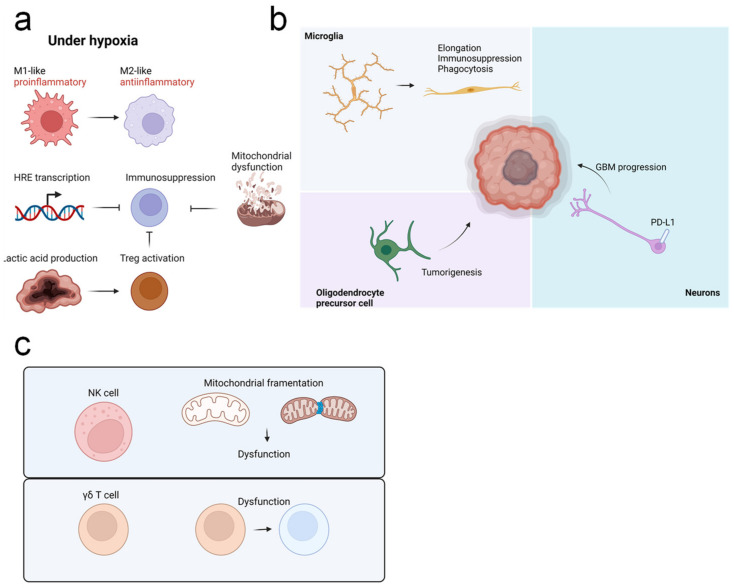
Hypoxia is a hallmark of glioblastoma multiforme (GBM), the most aggressive cancer of the central nervous system, and is associated with multiple aspects of tumor pathogenesis. For example, hypoxia induces resistance to conventional cancer therapies and inhibits antitumor immune responses. Thus, targeting hypoxia is an attractive strategy for GBM therapy. However, traditional studies on hypoxia have largely excluded the immune system. Recently, the critical role of the immune system in the defense against multiple tumors has become apparent, leading to the development of effective immunotherapies targeting numerous cancer types. Critically, however, GBM is classified as a "cold tumor" due to poor immune responses. Thus, to improve GBM responsiveness against immunotherapies, an improved understanding of both immune function in GBM and the role of hypoxia in mediating immune responses within the GBM microenvironment is needed. In this review, we discuss the role of hypoxia in GBM from a clinical, pathological, and immunological perspective.
Keywords: antitumor immunity; glioblastoma multiforme (GBM); hypoxia; immunotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
