

Timeline of Adverse Events during Immune Checkpoint Inhibitors for Advanced Melanoma and Their Impacts on Survival
- PMID: 35267545
- PMCID: PMC8909485
- DOI: 10.3390/cancers14051237
Timeline of Adverse Events during Immune Checkpoint Inhibitors for Advanced Melanoma and Their Impacts on Survival
Abstract
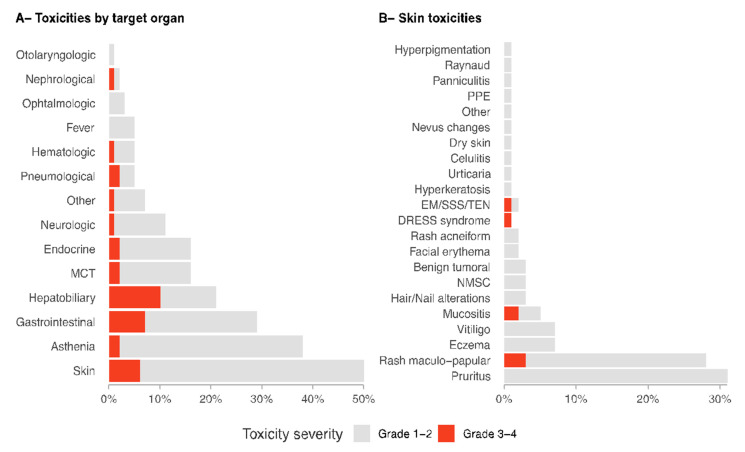
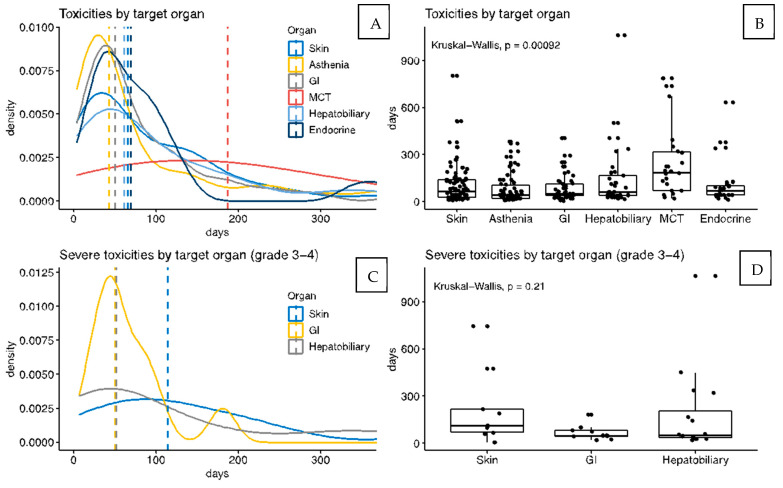
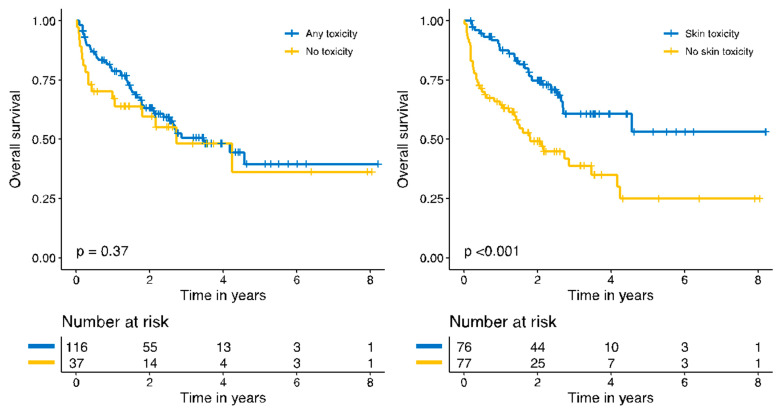
Immune-related adverse events (irAEs) are frequent and could be associated with improved response to immune checkpoint inhibitors (ICIs). A prospective cohort of advanced melanoma patients receiving ICI as first-line therapy was retrospectively reviewed (January 2011−February 2019). A total of 116 of 153 patients presented with at least one irAE (75.8%). The most frequent irAEs were dermatological (derm irAEs, 50%), asthenia (38%), and gastrointestinal (29%). Most irAEs appeared within the first 90 days, while 11.2% appeared after discontinuation of the therapy. Mild grade 1−2 derm irAEs tended to appear within the first 2 months of therapy with a median time of 65.5 days (IQR 26-139.25), while grade 3−4 derm irAEs appeared later (median 114 days; IQR 69-218) and could be detected at any time during therapy. Only derm irAE occurrence was related to improved survival (HR 6.46). Patients presenting derm irAEs showed better 5-year overall survival compared to those with no derm irAEs (53.1% versus 24.9%; p < 0.001). However, the difference was not significant when adjusting for the duration of therapy. In conclusion: the timeline of immune-related-AEs differs according to the organ involved. The (apparent) improved survival of patients who present derm AEs during immunotherapy could be partially explained by longer times under treatment.
Keywords: dermatological adverse events; dermatological drug reactions; immune checkpoint inhibitors; immune-related adverse events; immunotherapy; melanoma; outcome; survival.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Freeman-Keller M., Kim Y., Cronin H., Richards A., Gibney G., Weber J.S. Nivolumab in resected and unresectable metastatic melanoma: Characteristics of immune-related adverse events and association with outcomes. Clin. Cancer Res. 2016;22:886–894. doi: 10.1158/1078-0432.CCR-15-1136. - DOI - PMC - PubMed
-
- Hao C., Tian J., Tian J., Liu H., Li F., Niu H., Zhu B. Efficacy and safety of anti-PD-1 and anti-PD-1 combined with anti-CTLA-4 immunotherapy to advanced melanoma: A systematic review and meta-analysis of randomized controlled trials. Medicine. 2017;96:e7325. doi: 10.1097/MD.0000000000007325. - DOI - PMC - PubMed
-
- Schachter J., Ribas A., Long G.V., Arance A., Grob J.J., Mortier L., Daud A., Carlino M.S., McNeil C., Lotem M., et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006) Lancet. 2017;390:1853–1862. doi: 10.1016/S0140-6736(17)31601-X. - DOI - PubMed
-
- Duan J., Cui L., Zhao X., Bai H., Cai S., Wang G., Zhao Z., Zhao J., Chen S., Song J., et al. Use of Immunotherapy with Programmed Cell Death 1 vs Programmed Cell Death Ligand 1 Inhibitors in Patients with Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020;6:375–384. doi: 10.1001/jamaoncol.2019.5367. - DOI - PMC - PubMed
