

Association between Antibiotic Exposure and Systemic Immune Parameters in Cancer Patients Receiving Checkpoint Inhibitor Therapy
- PMID: 35267634
- PMCID: PMC8909108
- DOI: 10.3390/cancers14051327
Association between Antibiotic Exposure and Systemic Immune Parameters in Cancer Patients Receiving Checkpoint Inhibitor Therapy
Abstract
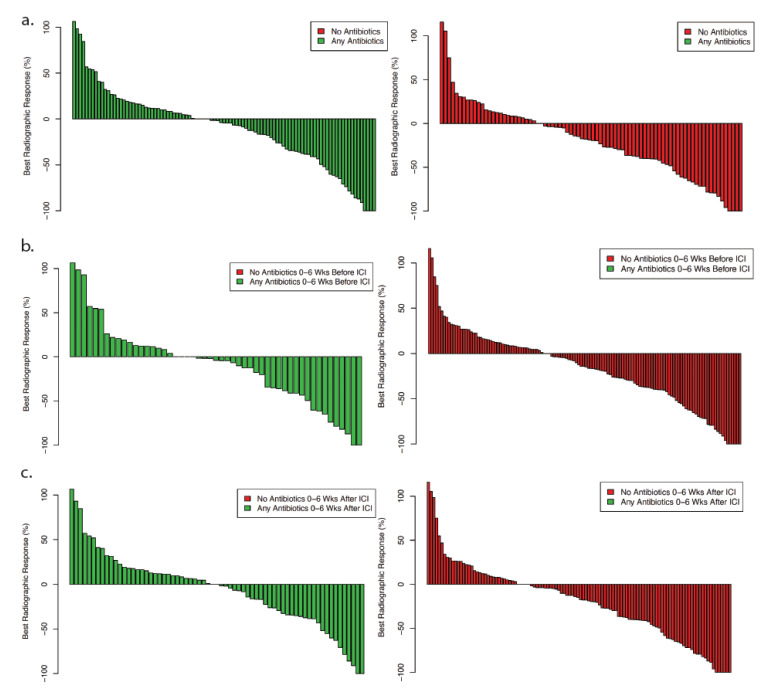
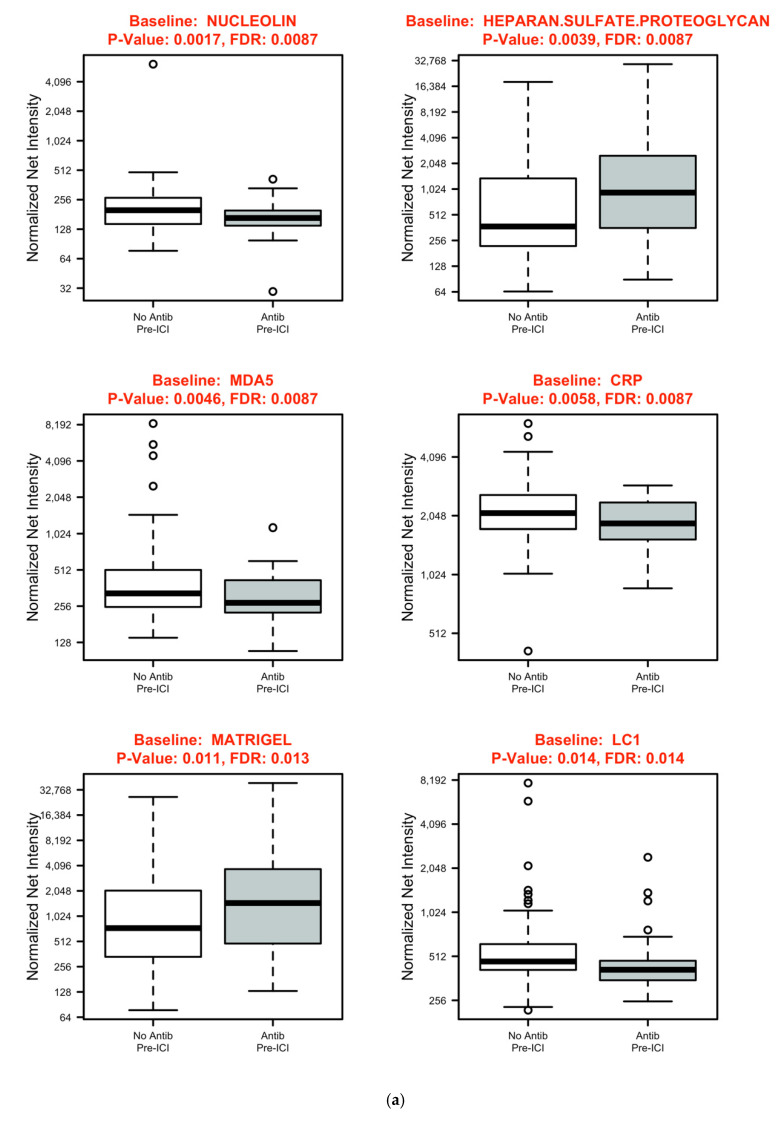
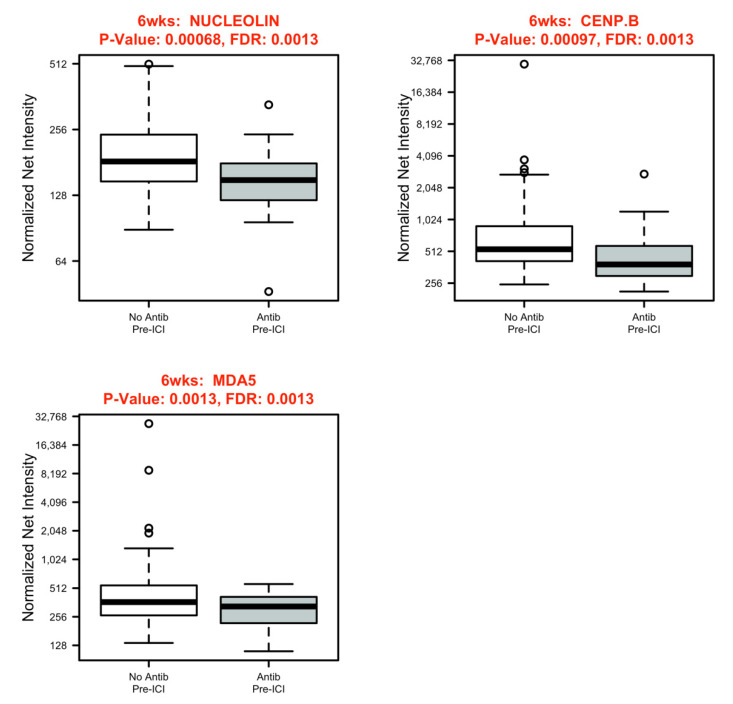
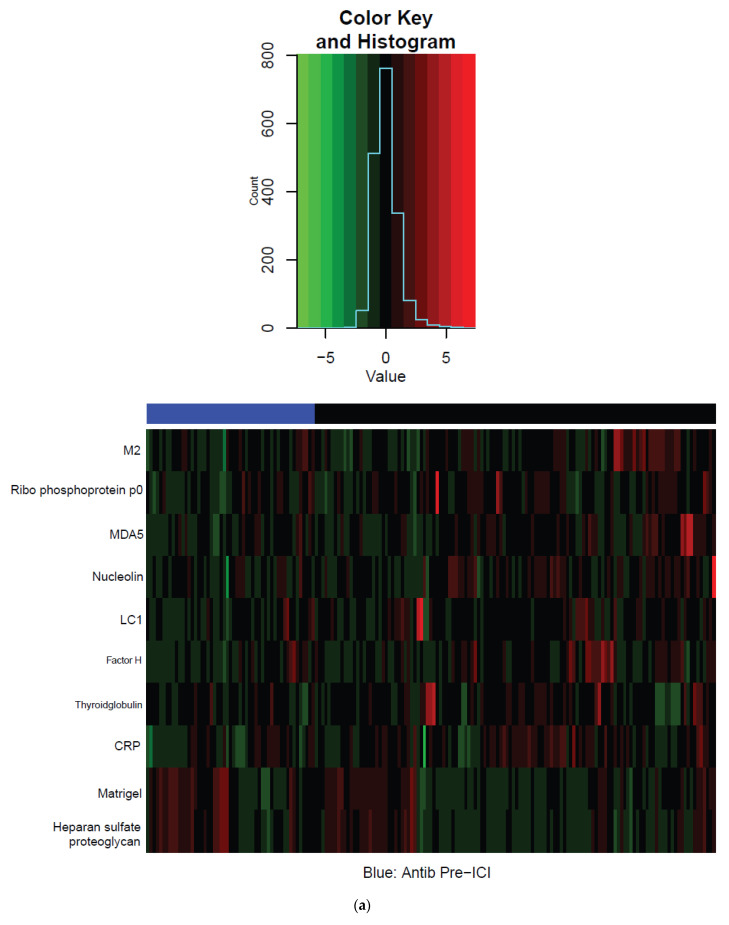
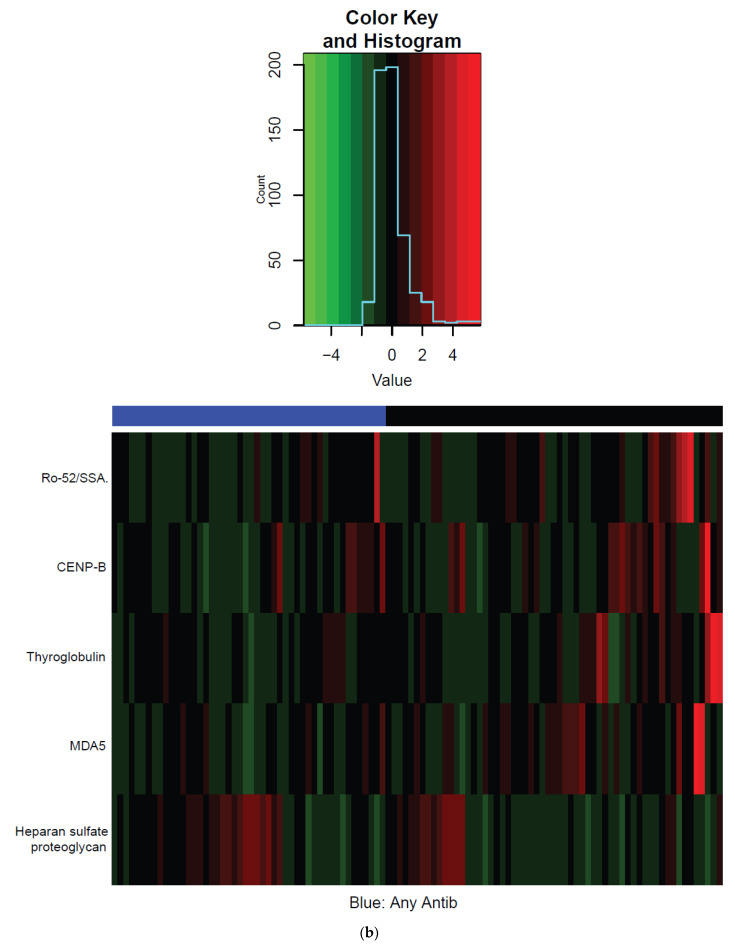
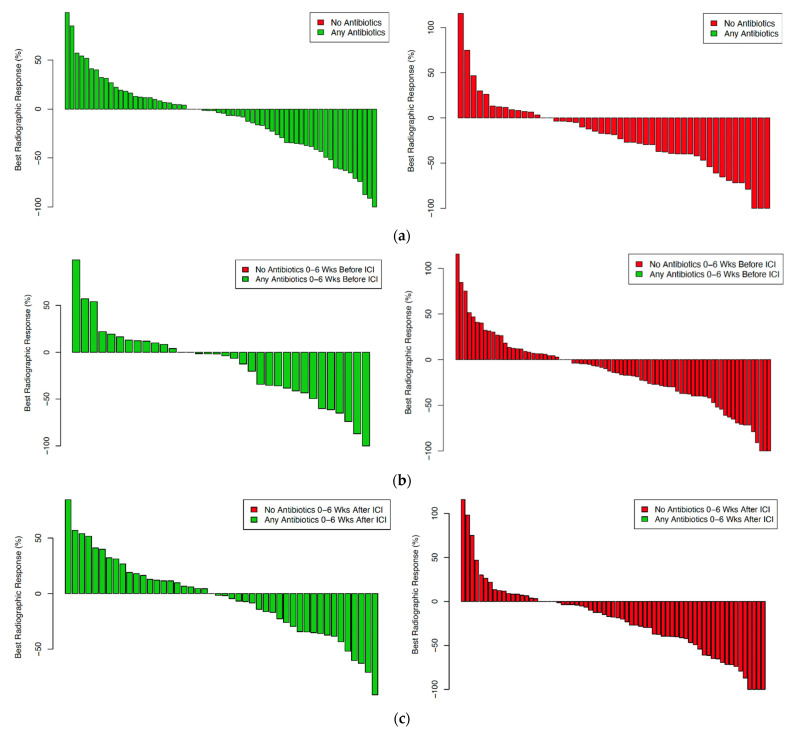
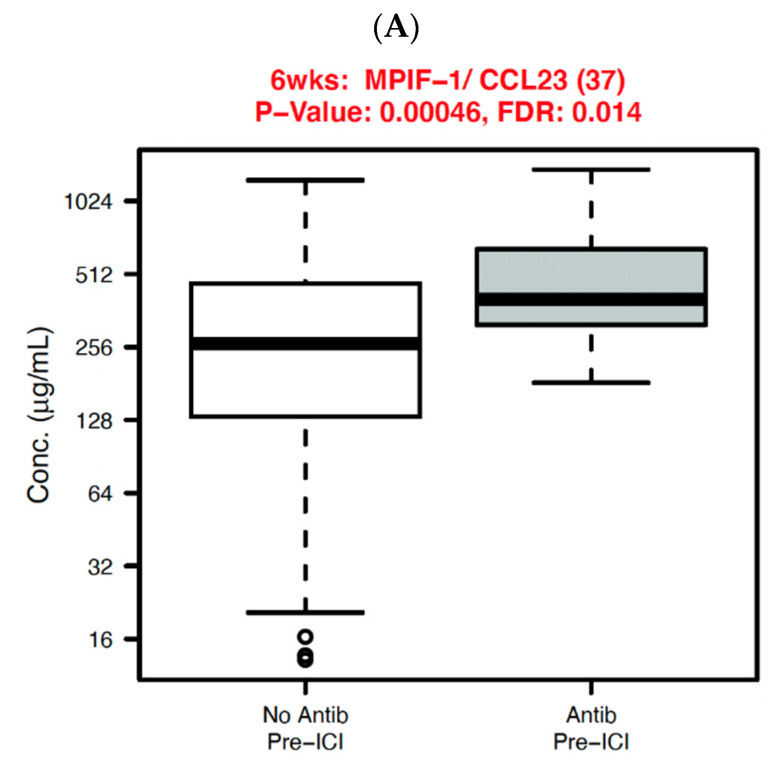
Antibiotic administration is associated with worse clinical outcomes and changes to the gut microbiome in cancer patients receiving immune checkpoint inhibitors (ICI). However, the effects of antibiotics on systemic immune function are unknown. We, therefore, evaluated antibiotic exposure, therapeutic responses, and multiplex panels of 40 serum cytokines and 124 antibodies at baseline and six weeks after ICI initiation, with p < 0.05 and false discovery rate (FDR) < 0.2 considered significant. A total of 251 patients were included, of whom the 135 (54%) who received antibiotics had lower response rates and shorter survival. Patients who received antibiotics prior to ICI initiation had modestly but significantly lower baseline levels of nucleolin, MDA5, c-reactive protein, and liver cytosol antigen type 1 (LC1) antibodies, as well as higher levels of heparin sulfate and Matrigel antibodies. After ICI initiation, antibiotic-treated patients had significantly lower levels of MDA5, CENP.B, and nucleolin antibodies. Although there were no clear differences in cytokines in the overall cohort, in the lung cancer subset (53% of the study population), we observed differences in IFN-γ, IL-8, and macrophage inflammatory proteins. In ICI-treated patients, antibiotic exposure is associated with changes in certain antibodies and cytokines. Understanding the relationship between these factors may improve the clinical management of patients receiving ICI.
Keywords: antibiotics; antibodies; biomarkers; cancer; cytokines; efficacy; immune checkpoint inhibitors; immunotherapy.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Overman M.J., Lonardi S., Wong K.Y.M., Lenz H.-J., Gelsomino F., Aglietta M., Morse M.A., Van Cutsem E., McDermott R., Hill A., et al. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair-Deficient/Microsatellite Instability-High Metastatic Colorectal Cancer. J. Clin. Oncol. 2018;36:773–779. doi: 10.1200/JCO.2017.76.9901. - DOI - PubMed
-
- Rizvi N.A., Hellmann M.D., Snyder A., Kvistborg P., Makarov V., Havel J.J., Lee W., Yuan J., Wong P., Ho T.S., et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348:124–128. doi: 10.1126/science.aaa1348. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
