

Evolution of Early Onset Scoliosis under Treatment with a 3D-Brace Concept
- PMID: 35268276
- PMCID: PMC8910874
- DOI: 10.3390/jcm11051186
Evolution of Early Onset Scoliosis under Treatment with a 3D-Brace Concept
Abstract
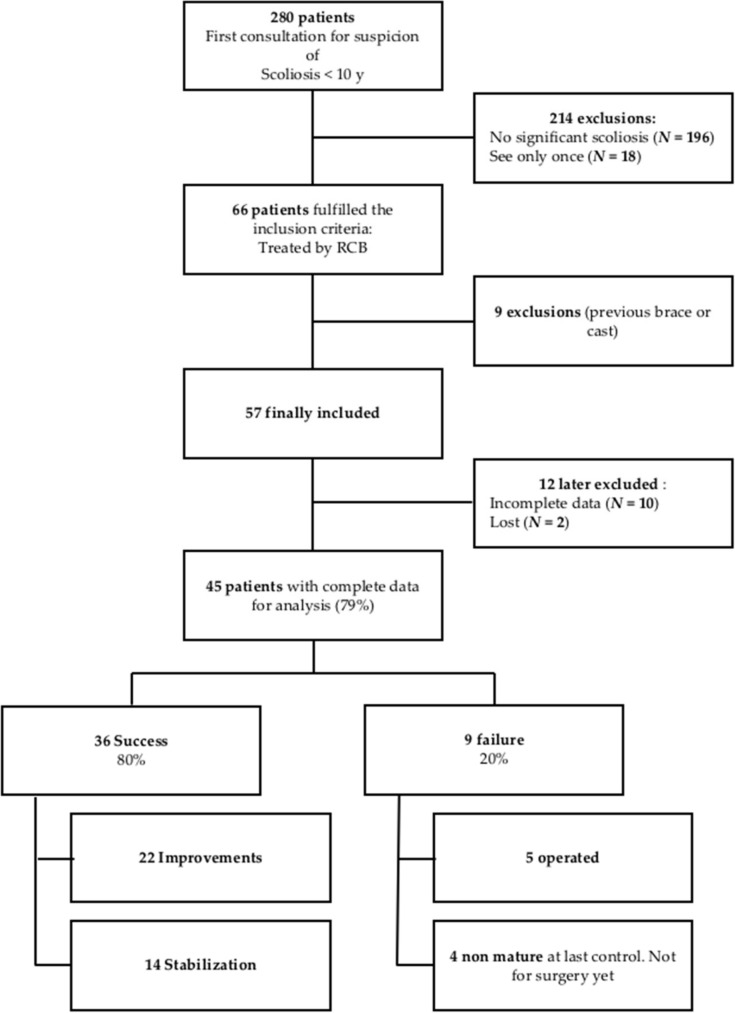
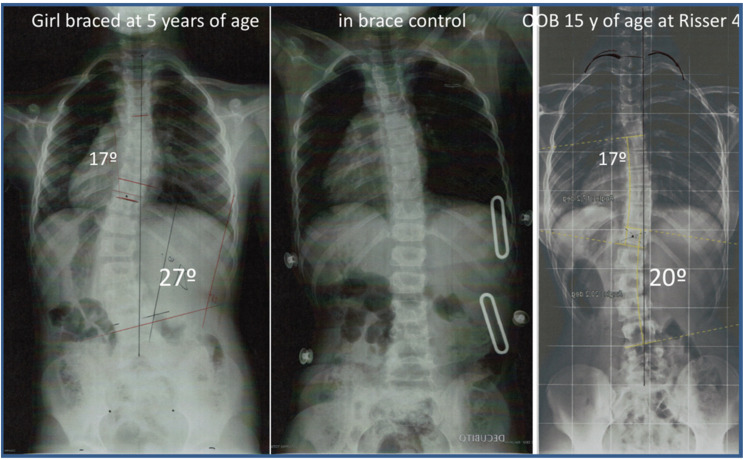
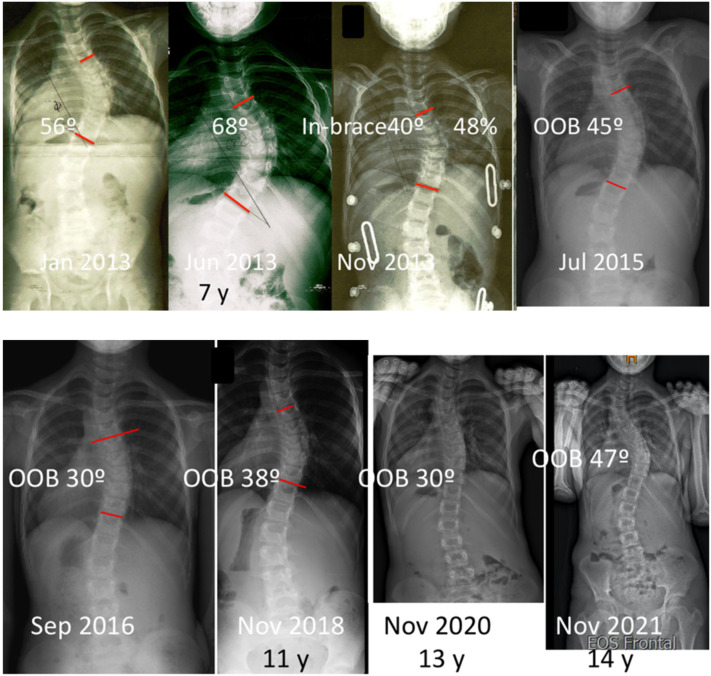
The objective of this study is to examine the evolution of all the braced patients diagnosed with early onset scoliosis in a private scoliosis center. All patients diagnosed with EOS and braced before the age of ten were retrospectively reviewed. The results have been defined in accordance with the Scoliosis Research Society (SRS) for bracing criteria, and with a minimum follow-up of one year. Improvement and stabilization were considered successful treatments, while failure was considered to be an unsuccessful treatment. Successful results were observed in 80% of patients (63% worst case). In the success group, the Cobb angle was reduced from 36.3° (21-68) to 25° (10-43), with 36% of patients being initially treated only with night-time bracing. Twenty percent of the patients failed, seven had more than 45° at the last control and five had undergone surgery. This study suggests that bracing, using a modern 3D-brace concept, could be an effective treatment option for early onset scoliosis and advocates exploring its effectiveness as an alternative to casting throughout studies of higher levels of evidence.
Keywords: bracing; early onset scoliosis; non-operative treatment.
Conflict of interest statement
R.S. declares no conflict of interest. M.R. declares: Honoraria for medical advice from Ortholutions (Germany) and from AlignClinic (California, USA). R.S. was an employee in the company Rigo Quera Salvá at the time the study was completed, working for the company until March 2020. Nowadays, R.S. is an employee of the French company UPNOS, working in the field of sleep disorders and also at Wandercraft, another French company, working in the field of exoskeletons. M.R. is an employer and director of the company Rigo Quera Salvá S.L.P., a private rehabilitation clinic for spinal deformities. All the braces were designed, manufactured and fitted in Ortopedia Grau Soler, Barcelona, Spain. M.R. personally designed all the braces. M.R. specifically declares that neither himself nor Rigo Quera Salvá S.L.P. have any type of commercial relationship, partnership, honoraria, direct or indirect incomes or benefits from Ortopedia Grau Soler.
Figures
Similar articles
-
Detorsion night-time bracing for the treatment of early onset idiopathic scoliosis.Orthop Traumatol Surg Res. 2014 Dec;100(8):935-9. doi: 10.1016/j.otsr.2014.05.024. Epub 2014 Nov 6. Orthop Traumatol Surg Res. 2014. PMID: 25459456
-
An Insight Into the Health-Related Quality of Life of Adolescent Idiopathic Scoliosis Patients Who Are Braced, Observed, and Previously Braced.Spine (Phila Pa 1976). 2019 May 15;44(10):E596-E605. doi: 10.1097/BRS.0000000000002918. Spine (Phila Pa 1976). 2019. PMID: 31046000
-
Curve Progression in Adolescent Idiopathic Scoliosis With a Minimum of 2 Years' Follow-up After Completed Brace Weaning With Reference to the SRS Standardized Criteria.Spine Deform. 2016 May;4(3):200-205. doi: 10.1016/j.jspd.2015.12.002. Epub 2016 Apr 16. Spine Deform. 2016. PMID: 27927503
-
Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management.Spine (Phila Pa 1976). 2005 Sep 15;30(18):2068-75; discussion 2076-7. doi: 10.1097/01.brs.0000178819.90239.d0. Spine (Phila Pa 1976). 2005. PMID: 16166897 Review.
-
Evolution of casting techniques in early-onset and congenital scoliosis.J Clin Orthop Trauma. 2020 Sep-Oct;11(5):810-815. doi: 10.1016/j.jcot.2020.06.034. Epub 2020 Jul 8. J Clin Orthop Trauma. 2020. PMID: 32879567 Free PMC article. Review.
Cited by
-
Effects of 3D Postural Correction and Abdominal Muscle Contraction on the Symmetry of the Transverse Abdominis and Spinal Alignment in Patients with Idiopathic Scoliosis.Int J Environ Res Public Health. 2023 Mar 12;20(6):5016. doi: 10.3390/ijerph20065016. Int J Environ Res Public Health. 2023. PMID: 36981926 Free PMC article.
-
Correlation of transverse rotation of the spine using surface topography and 3D reconstructive radiography in children with idiopathic scoliosis.Spine Deform. 2024 Jul;12(4):1001-1008. doi: 10.1007/s43390-024-00838-7. Epub 2024 Feb 26. Spine Deform. 2024. PMID: 38403800
-
Health technology assessment in musculoskeletal radiology: the case study of EOSedge™.Radiol Med. 2024 Jul;129(7):1076-1085. doi: 10.1007/s11547-024-01832-9. Epub 2024 Jun 10. Radiol Med. 2024. PMID: 38856961 Free PMC article.
References
-
- Revised Glossary of Terms | Scoliosis Research Society. [(accessed on 2 July 2019)]. Available online: https://www.srs.org/professionals/online-education-and-resources/glossar....
LinkOut - more resources
Full Text Sources
