

Diagnosis of Congenital Uterine Abnormalities: Practical Considerations
- PMID: 35268343
- PMCID: PMC8911320
- DOI: 10.3390/jcm11051251
Diagnosis of Congenital Uterine Abnormalities: Practical Considerations
Abstract
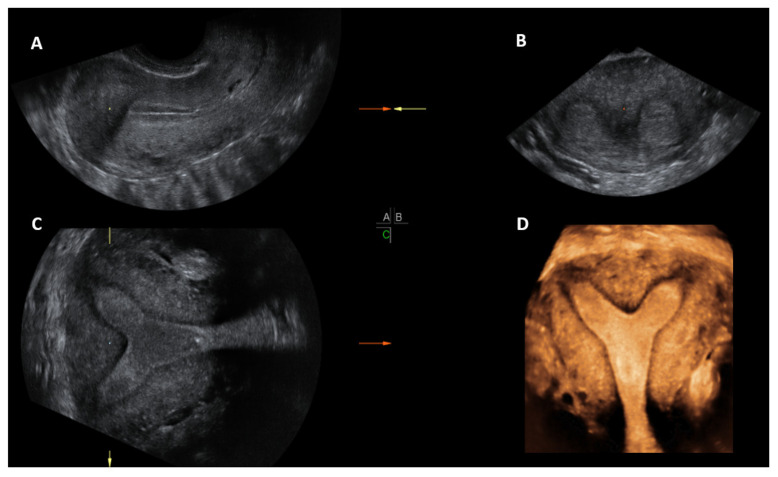
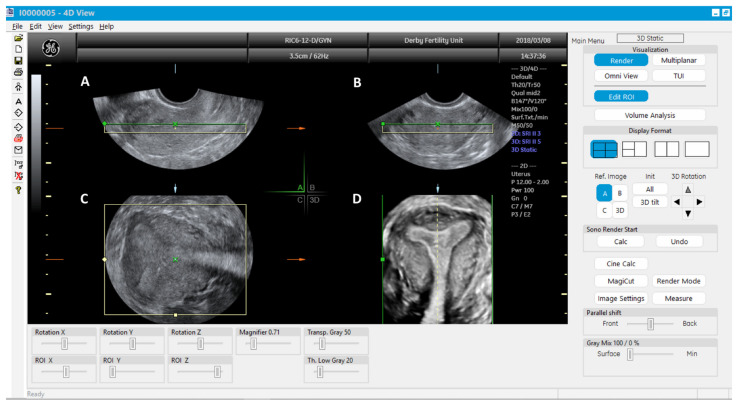
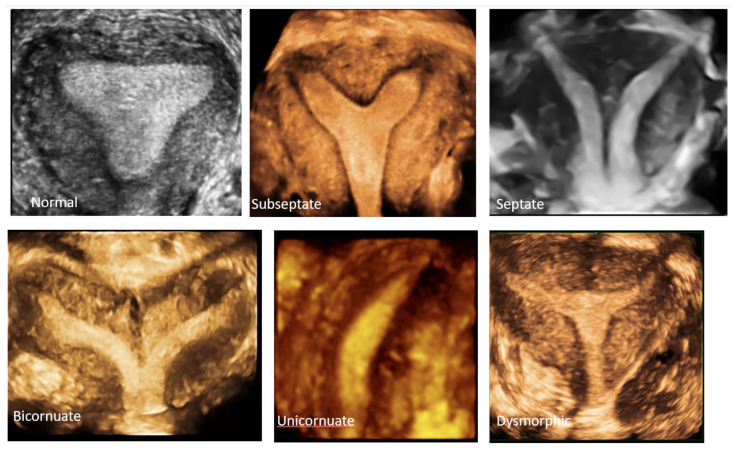
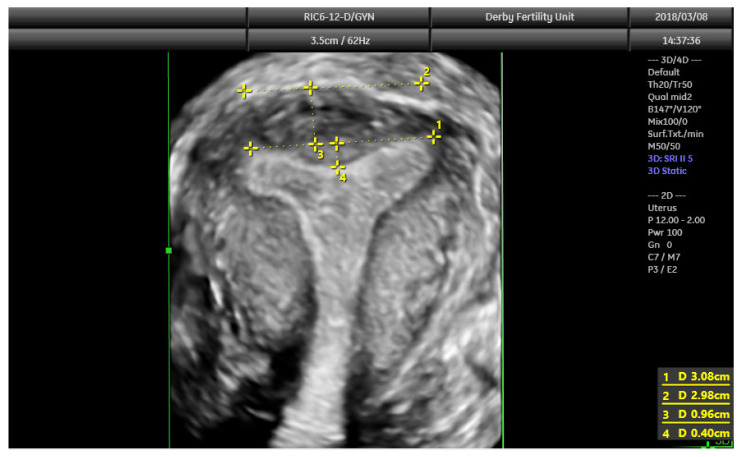
As most congenital uterine abnormalities are asymptomatic, the majority of them are detected incidentally. While most women with uterine anomalies have a normal reproductive outcome, some may experience adverse reproductive outcomes. Accurate diagnosis and correct classification help in the appropriate counselling of women about their potential reproductive prognosis and risks and for planning any intervention. Evaluation of the internal and external contours of the uterus is the key in making a diagnosis and correctly classifying a uterine anomaly. Considering this, the gold standard test has been the combined laparoscopy and hysteroscopy historically, albeit invasive. However, 3D ultrasound has now become the diagnostic modality of choice for uterine anomalies due to its high degree of diagnostic accuracy, less invasive nature and it being comparatively less expensive. While 2D ultrasound and HSG are adequate for screening for uterine anomalies, MRI and combined laparoscopy and hysteroscopy are reserved for diagnosing complex Mullerian anomalies. Imaging for renal anomalies is recommended if a uterine anomaly is diagnosed.
Keywords: 3D ultrasound; MRI; Mullerian duct; congenital uterine anomalies; diagnosis; hysteroscopy; laparoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
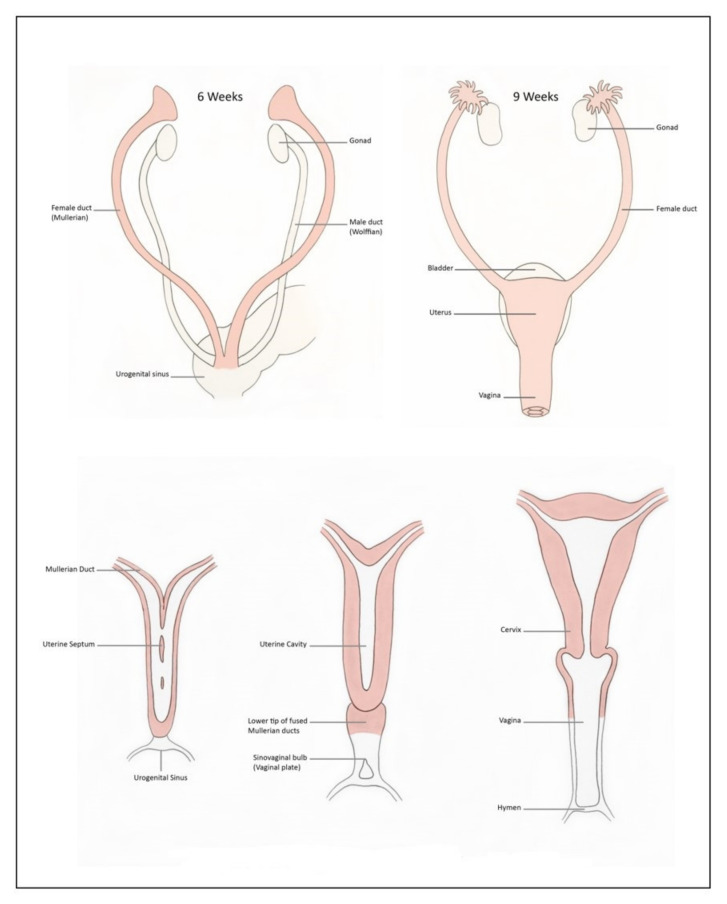
- Sadler T.W. Langman’s Medical Embryology. 12th ed. Lippincott Williams & Wilkins; Philadelphia, PA, USA: 2012. pp. 243–259.
-
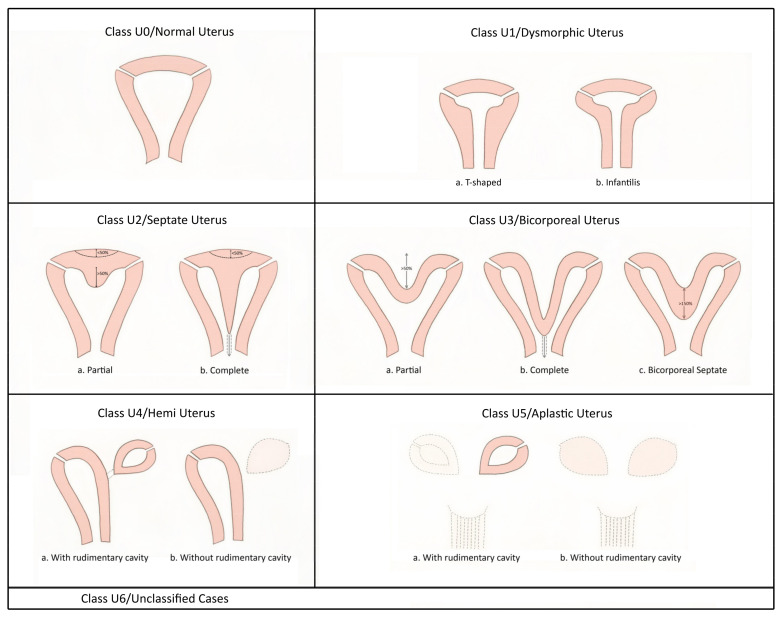
- AFS. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil. Steril. 1988;49:944–955. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
