

Minimally Invasive Partial vs. Total Adrenalectomy for the Treatment of Unilateral Primary Aldosteronism: A Systematic Review and Meta-Analysis
- PMID: 35268355
- PMCID: PMC8911420
- DOI: 10.3390/jcm11051263
Minimally Invasive Partial vs. Total Adrenalectomy for the Treatment of Unilateral Primary Aldosteronism: A Systematic Review and Meta-Analysis
Abstract
Background: This systematic review and metanalysis was conducted to assess differences between perioperative and functional outcomes in patients undergoing minimally-invasive partial (mi-PA) and total adrenalectomy (mi-TA) for unilateral primary aldosteronism (uPHA).
Material and methods: Multiple scientific databases (PUBMED, Web of Science, and Cochrane Library) were searched up to November 2021 for surgical series comparing mi-PA vs. mi-TA for uPHA according to the PRISMA statement. Primary outcomes of interest were perioperative and functional outcomes.
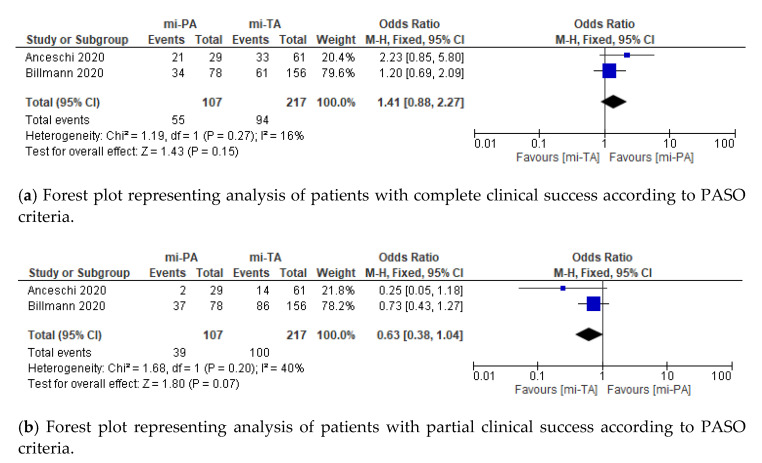
Results: Overall, a total of 802 patients from six eligible studies were identified, with mi-PA and mi-TA performed in 40.4% (n = 324) and 59.6% (n = 478) of cases, respectively. No differences were recorded between the two groups according to number of transfusions, EBL and Clavien-Dindo complications ≥2. Similarly, no differences in clinical success, persistence of postoperative hypokalemia and improvement in HTN were reported between mi-PA and mi-TA.
Conclusions: In a uPHA setting, mi-PA and mi-TA provide comparable perioperative and functional outcomes despite the use of mi-PA remains limited to patients with small adenoma size, or hereditary/bilateral disease. Due to limited use of standardized reporting criteria in most of current series, the quest for a superiority of mi-PA over mi-TA in the treatment of uPHA still remains open.
Keywords: Conn’s syndrome; PASO; partial adrenalectomy; total adrenalectomy; unilateral primary aldosteronism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





Similar articles
-
Clinical cure vs a novel trifecta system for evaluating long-term outcomes of minimally-invasive partial or total adrenalectomy for unilateral primary aldosteronism: results of a multicentric series.Cent European J Urol. 2022;75(4):345-351. doi: 10.5173/ceju.2022.147. Epub 2022 Oct 18. Cent European J Urol. 2022. PMID: 36794029 Free PMC article.
-
Minimally Invasive Partial Versus Total Adrenalectomy for the Treatment of Primary Aldosteronism: Results of a Multicenter Series According to the PASO Criteria.Eur Urol Focus. 2021 Nov;7(6):1418-1423. doi: 10.1016/j.euf.2020.06.023. Epub 2020 Jul 11. Eur Urol Focus. 2021. PMID: 32660839
-
Partial versus total adrenalectomy for the treatment of unilateral aldosterone-producing adenoma: a systematic review and meta-analysis.Updates Surg. 2021 Dec;73(6):2301-2313. doi: 10.1007/s13304-021-01116-1. Epub 2021 Jun 19. Updates Surg. 2021. PMID: 34148213
-
Robot-assisted Partial Adrenalectomy for the Treatment of Conn's Syndrome: Surgical Technique, and Perioperative and Functional Outcomes.Eur Urol. 2019 May;75(5):811-816. doi: 10.1016/j.eururo.2018.07.030. Epub 2018 Aug 1. Eur Urol. 2019. PMID: 30077398
-
Approach to the surgical management of primary aldosteronism.Gland Surg. 2015 Feb;4(1):69-81. doi: 10.3978/j.issn.2227-684X.2015.01.05. Gland Surg. 2015. PMID: 25713782 Free PMC article. Review.
Cited by
-
Retroperitoneoscopic enucleation adrenalectomy: a viable surgical option for small nonsecreting adrenal tumors with low potential of malignancy.Transl Androl Urol. 2023 Nov 30;12(11):1713-1722. doi: 10.21037/tau-23-54. Epub 2023 Nov 16. Transl Androl Urol. 2023. PMID: 38106691 Free PMC article.
-
Clinical cure vs a novel trifecta system for evaluating long-term outcomes of minimally-invasive partial or total adrenalectomy for unilateral primary aldosteronism: results of a multicentric series.Cent European J Urol. 2022;75(4):345-351. doi: 10.5173/ceju.2022.147. Epub 2022 Oct 18. Cent European J Urol. 2022. PMID: 36794029 Free PMC article.
-
Cost-effectiveness analysis of segmental adrenal venous sampling with radiofrequency ablation for primary aldosteronism in Japan.Jpn J Radiol. 2025 Feb;43(2):290-300. doi: 10.1007/s11604-024-01665-6. Epub 2024 Sep 25. Jpn J Radiol. 2025. PMID: 39317867 Free PMC article.
-
Recurrence of primary aldosteronism 20 years after surgery: a case report.J Hum Hypertens. 2025 Mar;39(3):237-239. doi: 10.1038/s41371-025-00994-x. Epub 2025 Feb 20. J Hum Hypertens. 2025. PMID: 39972196 No abstract available.
-
Treating Primary Aldosteronism-Induced Hypertension: Novel Approaches and Future Outlooks.Endocr Rev. 2024 Jan 4;45(1):125-170. doi: 10.1210/endrev/bnad026. Endocr Rev. 2024. PMID: 37556722 Free PMC article.
References
-
- Rossi G.P., Bernini G., Caliumi C., Desideri G., Fabris B., Ferri C., Ganzaroli C., Giacchetti G., Letizia C., Maccario M., et al. A Prospective Study of the Prevalence of Primary Aldosteronism in 1,125 Hypertensive Patients. J. Am. Coll. Cardiol. 2006;48:2293–2300. doi: 10.1016/j.jacc.2006.07.059. - DOI - PubMed
-
- Mulatero P., Stowasser M., Loh K.C., Fardella C.E., Gordon R.D., Mosso L., Gomez-Sanchez C.E., Veglio F., Young W.F. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J. Clin. Endocrinol. Metab. 2004;89:1045–1050. doi: 10.1210/jc.2003-031337. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
