

Developing a Mechanistic Approach to Sudden Death Prevention in Mitral Valve Prolapse
- PMID: 35268384
- PMCID: PMC8910972
- DOI: 10.3390/jcm11051285
Developing a Mechanistic Approach to Sudden Death Prevention in Mitral Valve Prolapse
Abstract
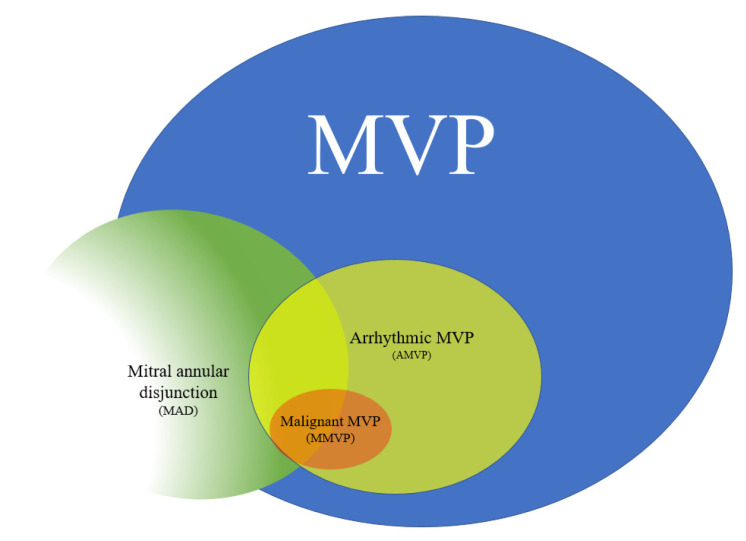
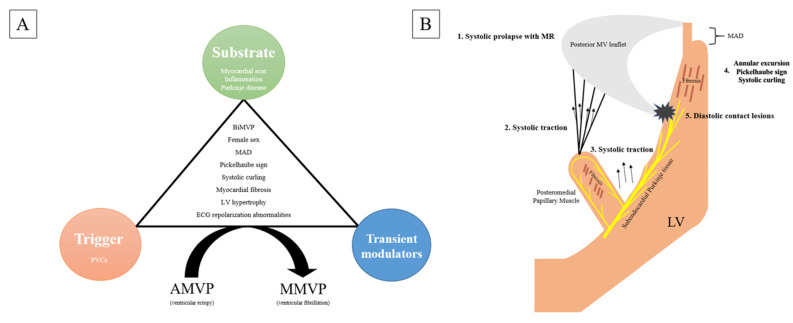
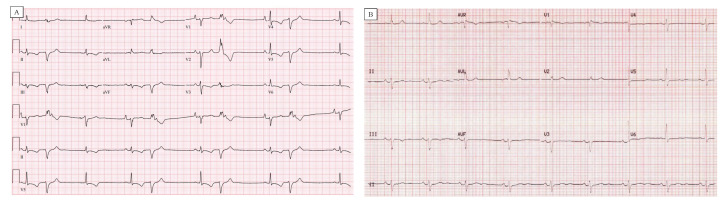
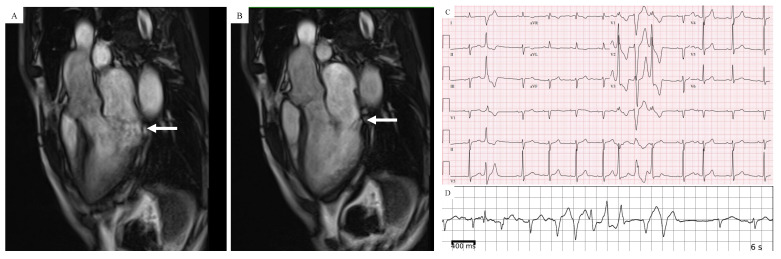
Sudden cardiac death (SCD) from ventricular fibrillation (VF) can occur in mitral valve prolapse (MVP) in the absence of other comorbidities including mitral regurgitation, heart failure or coronary disease. Although only a small proportion with MVP are at risk, it can affect young, otherwise healthy adults, most commonly premenopausal women, often as the first presentation of MVP. In this review, we discuss arrhythmic mechanisms in MVP and mechanistic approaches for sudden death risk assessment and prevention. We define arrhythmogenic or arrhythmic MVP (AMVP) as MVP associated with complex and frequent ventricular ectopy, and malignant MVP (MMVP) as MVP with high risk of SCD. Factors predisposing to AMVP are myxomatous, bileaflet MVP and mitral annular disjunction (MAD). Data from autopsy, cardiac imaging and electrophysiological studies suggest that ectopy in AMVP is due to inflammation, fibrosis and scarring within the left ventricular (LV) base, LV papillary muscles and Purkinje tissue. Postulated mechanisms include repetitive injury to these regions from systolic papillary muscle stretch and abrupt mitral annular dysmotility (excursion and curling) and diastolic endocardial interaction of redundant mitral leaflets and chordae. Whereas AMVP is seen relatively commonly (up to 30%) in those with MVP, MVP-related SCD is rare (2-4%). However, the proportion at risk (i.e., with MMVP) is unknown. The clustering of cardiac morphological and electrophysiological characteristics similar to AMVP in otherwise idiopathic SCD suggests that MMVP arises when specific arrhythmia modulators allow for VF initiation and perpetuation through action potential prolongation, repolarization heterogeneity and Purkinje triggering. Adequately powered prospective studies are needed to assess strategies for identifying MMVP and the primary prevention of SCD, including ICD implantation, sympathetic modulation and early surgical mitral valve repair. Given the low event rate, a collaborative multicenter approach is essential.
Keywords: mitral regurgitation; mitral valve prolapse; sudden cardiac death; ventricular arrhythmia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
