

Locomotive Syndrome and Lumbar Spine Disease: A Systematic Review
- PMID: 35268395
- PMCID: PMC8911455
- DOI: 10.3390/jcm11051304
Locomotive Syndrome and Lumbar Spine Disease: A Systematic Review
Abstract
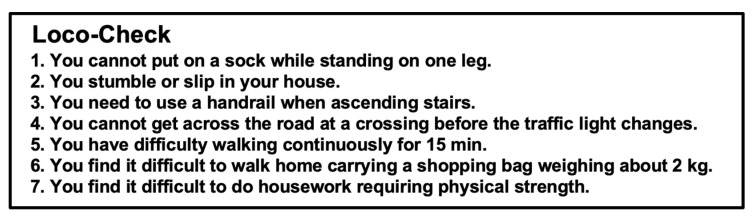
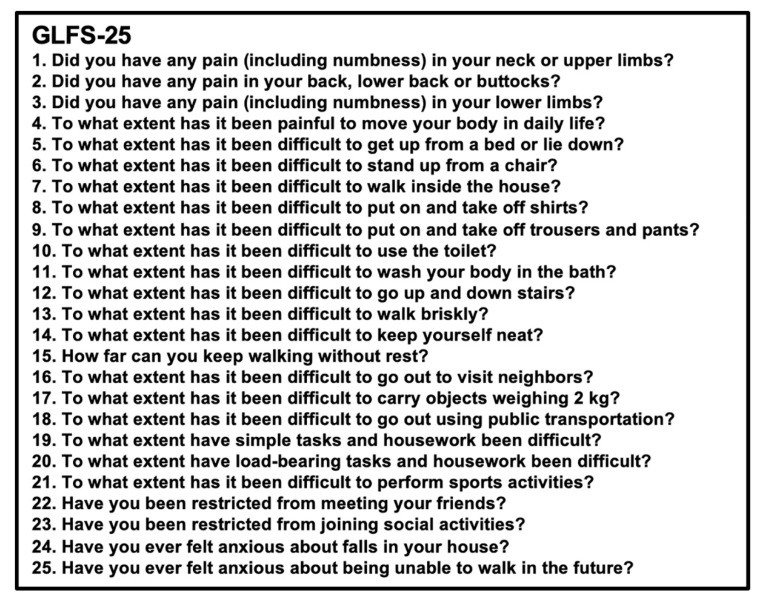
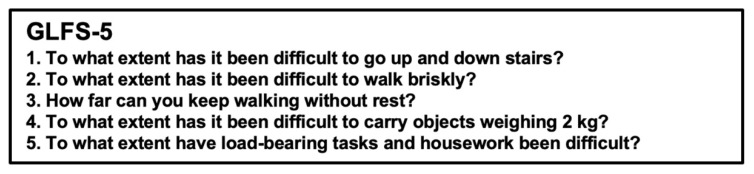
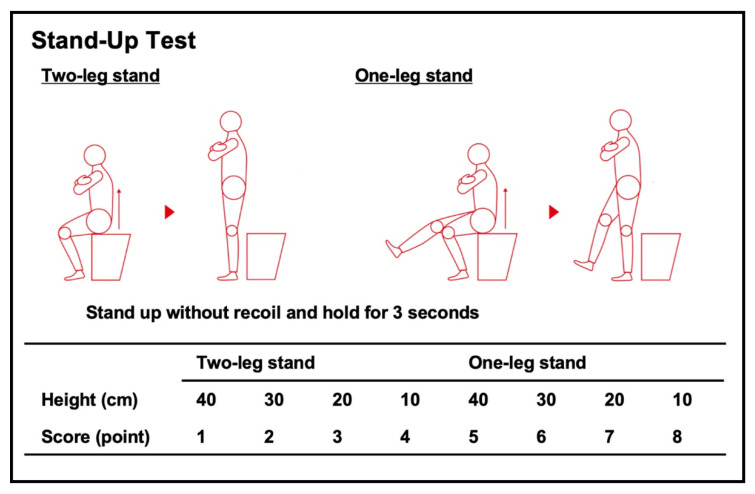
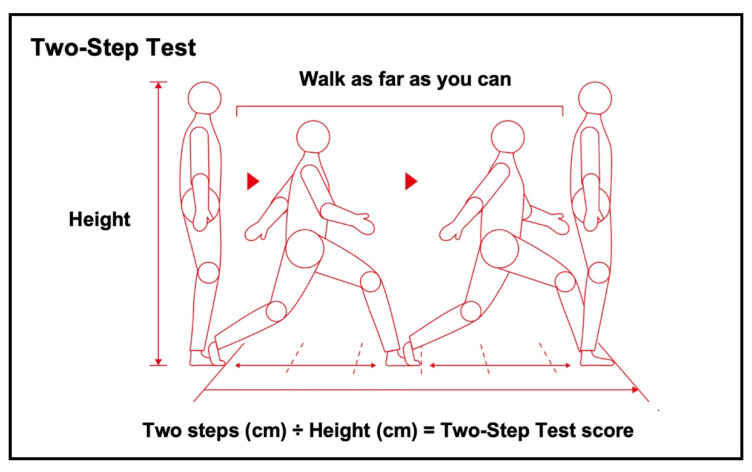
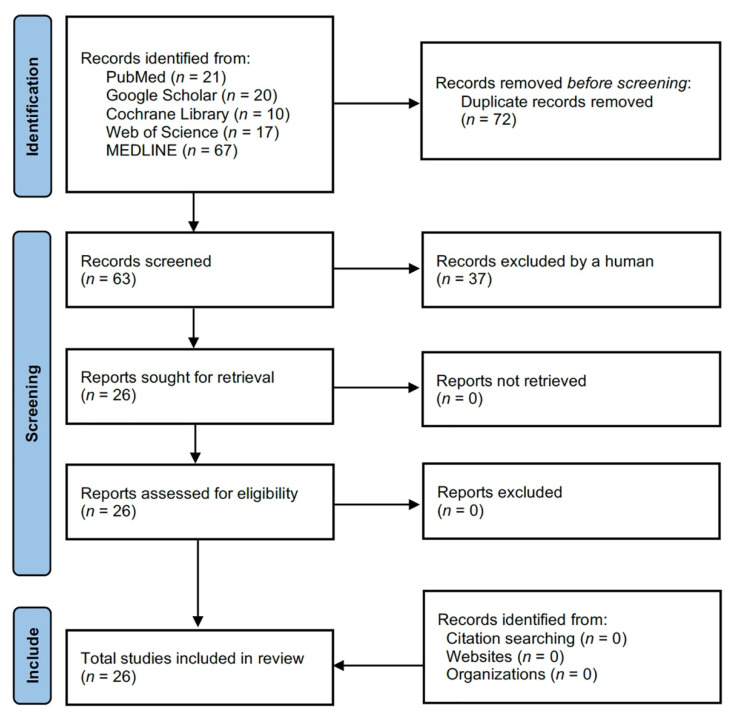
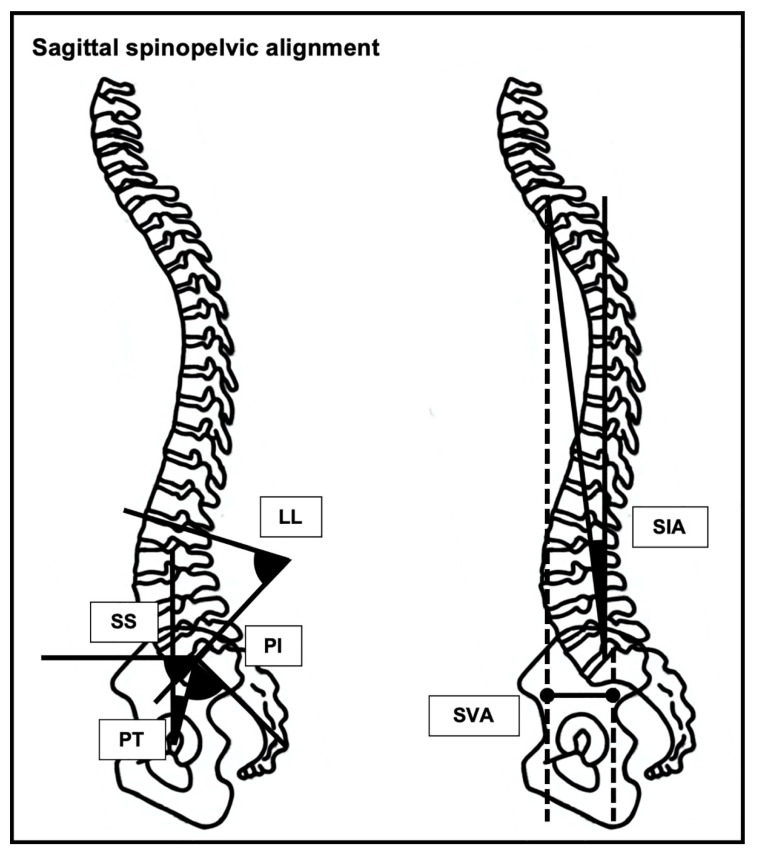
Locomotive syndrome (LS) is defined based on the Loco-Check, 25-question Geriatric Locomotive Function Scale (GLFS-25), 5-question Geriatric Locomotive Function Scale (GLFS-5), Stand-Up Test, Two-Step Test, or a total assessment (i.e., positive for one or more of the GLFS-25, Stand-Up Test, and Two-Step Test). Lumbar spine disease has been reported to be one of the most common musculoskeletal disorders leading to LS. We therefore conducted a systematic review via PubMed, Google Scholar, Cochrane Library, Web of Science, and MEDLINE, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A total of 26 studies were considered to be eligible for inclusion in this systematic review. The GLFS-25 showed an association with low back pain, sagittal spinopelvic malalignment, and lumbar spinal stenosis but not vertebral fracture. The GLFS-5 showed an association with low back pain and lumbar spinal stenosis. The Loco-Check and Two-Step Test showed an association with low back pain, sagittal spinopelvic malalignment, and lumbar spinal stenosis. The Stand-Up Test showed no association with lumbar spinal stenosis. The total assessment showed an association with low back pain and lumbar spinal stenosis. Furthermore, the GLFS-25, Two-Step Test, and total assessment were improved by spinal surgery for lumbar spinal stenosis. The current evidence concerning the relationship between LS and lumbar spine disease still seems insufficient, so further investigations are required on this topic.
Keywords: 25-question Geriatric Locomotive Function Scale; 5-question Geriatric Locomotive Function Scale; Loco-Check; Stand-Up Test; Two-Step Test; locomotive syndrome; lumbar spine.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- The Ministry of Internal Affairs and Communications. [(accessed on 15 February 2022)]. Available online: https://www.mhlw.go.jp/toukei/list/81-1a.html.
Publication types
LinkOut - more resources
Full Text Sources
