

Graft Failure Due to Nonadherence among 150 Prospectively-Followed Kidney Transplant Recipients at 18 Years Post-transplant: Our Results and Review of the Literature
- PMID: 35268424
- PMCID: PMC8911343
- DOI: 10.3390/jcm11051334
Graft Failure Due to Nonadherence among 150 Prospectively-Followed Kidney Transplant Recipients at 18 Years Post-transplant: Our Results and Review of the Literature
Abstract
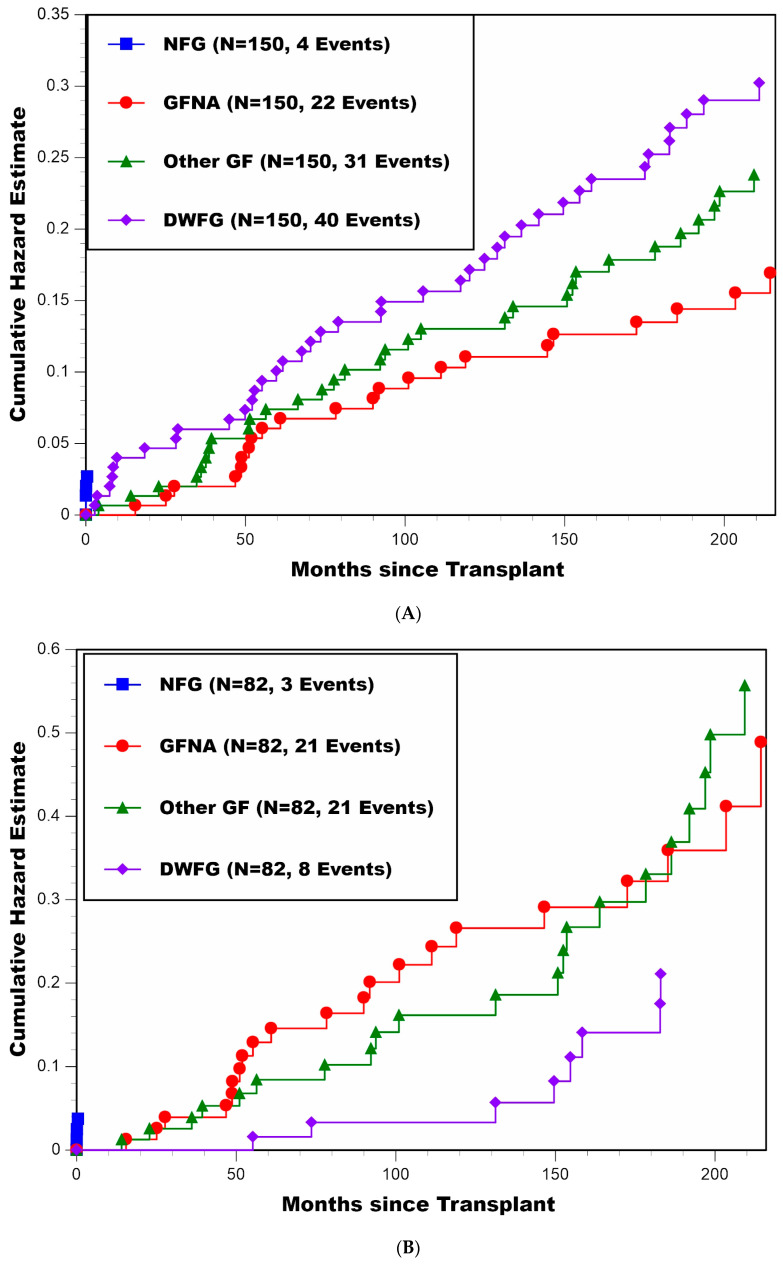
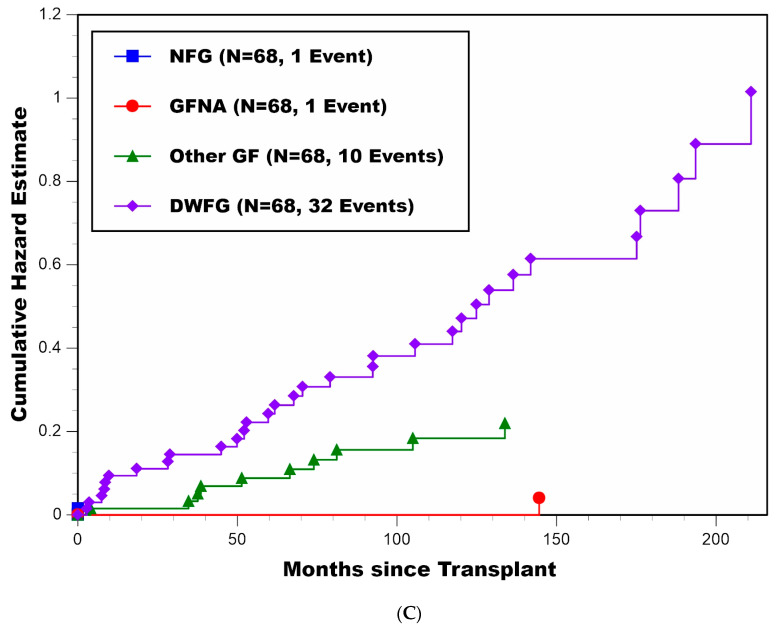
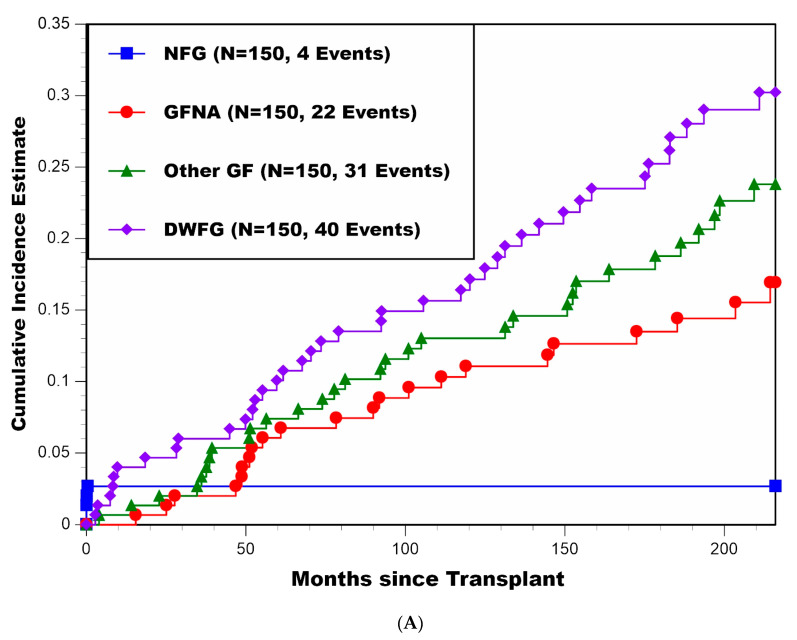
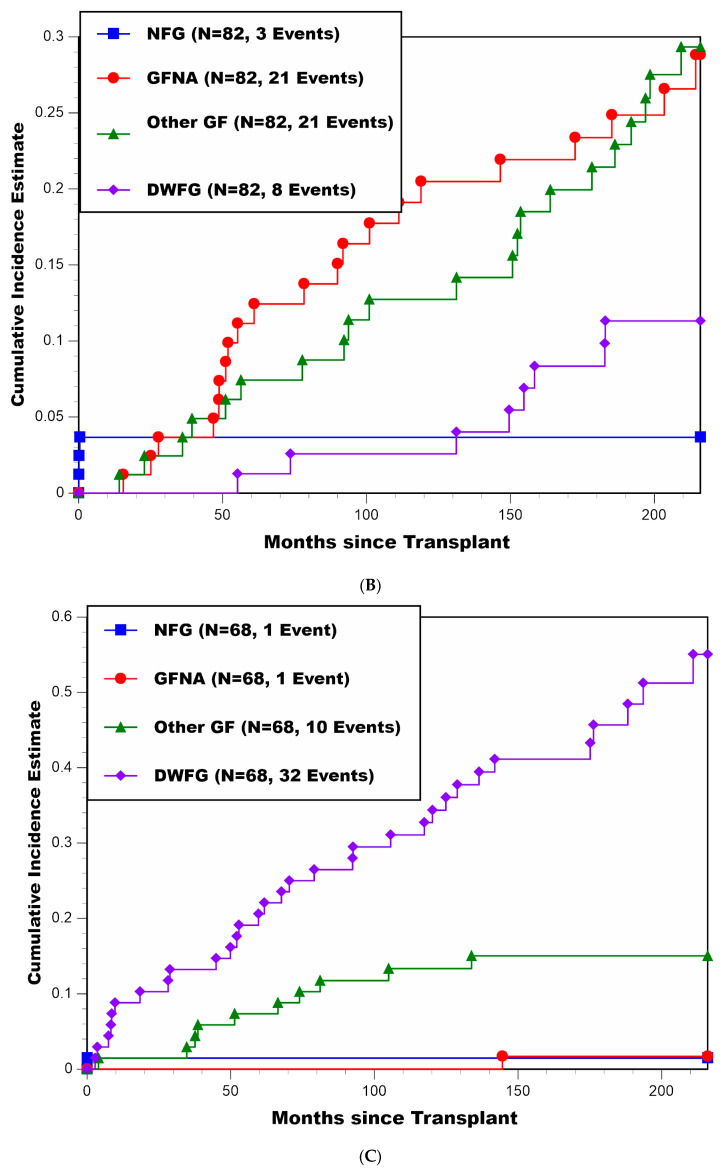
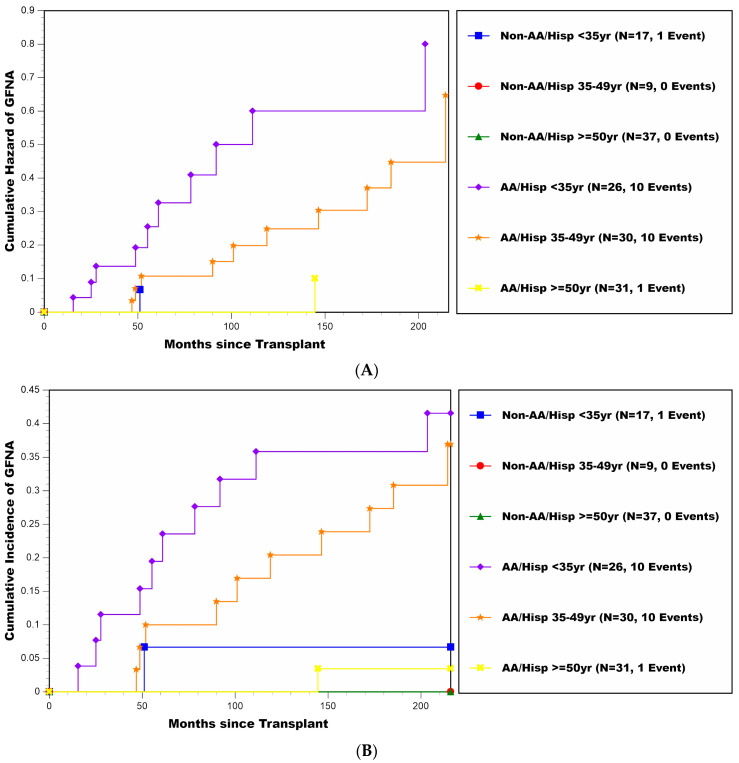
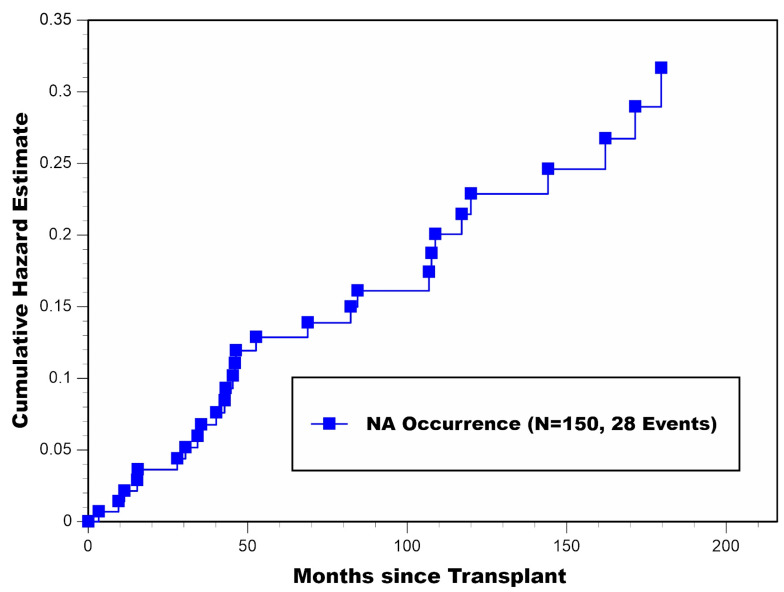
Background: We previously reported that graft failure due to nonadherence (GFNA) was a major cause of graft loss in kidney transplantation. Here, among 150 prospectively-followed kidney transplant recipients at 18 years post-transplant, we provide: updated (longer-term) estimates of cause-specific graft loss probabilities, risk factors for developing GFNA, and detailed characterizations of patients’ overt nonadherent (NA) behavior, including timing, extent, and clinical consequences. Methods: Determination of the patient becoming NA in taking his/her immunosuppressive medications, and the underlying cause of graft loss, were determined prospectively by the attending physicians. For never-functioning-graft, GFNA, GF due to causes other than NA (Other GF), and death with a functioning graft (DWFG), cumulative incidence functions were used to estimate the cumulative probabilities of cause-specific graft loss. Cox stepwise regression was used to determine significant multivariable predictors for the hazard rate of developing GFNA. Results: GFNA was a major cause of graft loss (22/150 patients), particularly among African-American and Hispanic recipients <50 years of age-at-transplant (20/56 experienced GFNA), with estimated percentages of such patients ever developing GFNA ranging between 36.9 and 41.5%. These patients were also at a higher risk of developing Other GF. For the remaining patients (2/94 experienced GFNA), estimated percentages of ever-developing GFNA were much lower (range: 0.0−6.7%). The major cause of graft loss among recipients ≥50 years of age was DWFG; GFNA rarely occurred among older recipients. In 21/22 GFNA patients, NA behavior lasted continuously from the time of developing NA until GFNA. In total, 28/150 patients became NA, and 67.9% (19/28) occurred beyond 36 months post-transplant. A total of 25 of 28 NA patients (89.3%) developed biopsy-proven acute rejection and/or chronic rejection that was directly attributed to the NA behavior. Lastly, 25/28 admitted to NA behavior, with financial and psychological components documented in 71.4% (20/28) and 96.4% (27/28) of NA cases, respectively. Conclusions: These results highlight the importance of performing serial monitoring of patients for overt NA behavior throughout their post-transplant follow-up. Financial and psychological components to NA behavior need to be simultaneously addressed with the goal of achieving complete avoidance/elimination of NA behavior among higher risk patients.
Keywords: 18-year prospective cohort study; cause-specific graft loss estimates; graft failure due to nonadherence; kidney transplantation; overt nonadherence; prognostic factors.
Conflict of interest statement
The authors declare no conflict of interest. The authors declare that the results presented in this paper have not been published previously in whole or part, except in abstract format.
Figures
References
-
- Gaynor J.J., Ciancio G., Guerra G., Sageshima J., Hanson L., Roth D., Chen L., Kupin W., Mattiazzi A., Tueros L., et al. Graft failure due to noncompliance among 628 kidney transplant recipients with long-term follow-up: A single-center observational study. Transplantation. 2014;97:925–933. doi: 10.1097/01.TP.0000438199.76531.4a. - DOI - PubMed
-
- Didlake R.H., Dreyfus K., Kerman R.H., Van Buren C.T., Kahan B.D. Patient noncompliance: A major cause of late graft failure in cyclosporine-treated renal transplants. Transplant. Proc. 1988;20:63–69. - PubMed
-
- Bergmann L.S., Roper L., Bow L.M., Hull D., Bartus S.A., Schweizer R.T. Causes of late graft failure in cadaveric renal transplantation. Transplant. Proc. 1993;25:1340–1341. - PubMed
LinkOut - more resources
Full Text Sources
