

Predicting the Need for Renal Replacement Therapy Using a Vascular Occlusion Test and Tissue Oxygen Saturation in Patients in the Early Phase of Multiorgan Dysfunction Syndrome
- PMID: 35268511
- PMCID: PMC8911273
- DOI: 10.3390/jcm11051420
Predicting the Need for Renal Replacement Therapy Using a Vascular Occlusion Test and Tissue Oxygen Saturation in Patients in the Early Phase of Multiorgan Dysfunction Syndrome
Abstract
Background: Acute kidney injury (AKI) is associated with an increased mortality in critically ill patients, especially in patients with multiorgan dysfunction syndrome (MODS). In daily clinical practice, the grading of AKI follows the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. In most cases, a relevant delay occurs frequently between the onset of AKI and detectable changes in creatinine levels as well as clinical symptoms. The aim of the present study was to examine whether a near infrared spectroscopy (NIRS)-based, non-invasive ischemia-reperfusion test (vascular occlusion test (VOT)) together with unprovoked (under resting conditions) tissue oxygen saturation (StO2) measurements, contain prognostic information in the early stage of MODS regarding the developing need for renal replacement therapy (RRT).
Methods: Within a period of 18 months, patients at the medical intensive care unit of a tertiary university hospital with newly developed MODS (≤24 h after diagnosis, APACHE II score ≥20) were included in our study. The VOT occlusion slope (OS) and recovery slope (RS) were recorded in addition to unprovoked StO2. StO2 was determined non-invasively in the area of the thenar muscles using a bedside NIRS device. The VOT was carried out by inflating a blood pressure cuff on the upper arm. AKI stages were determined by the changes in creatinine levels, urinary output, and/or the need for RRT according to KDIGO.
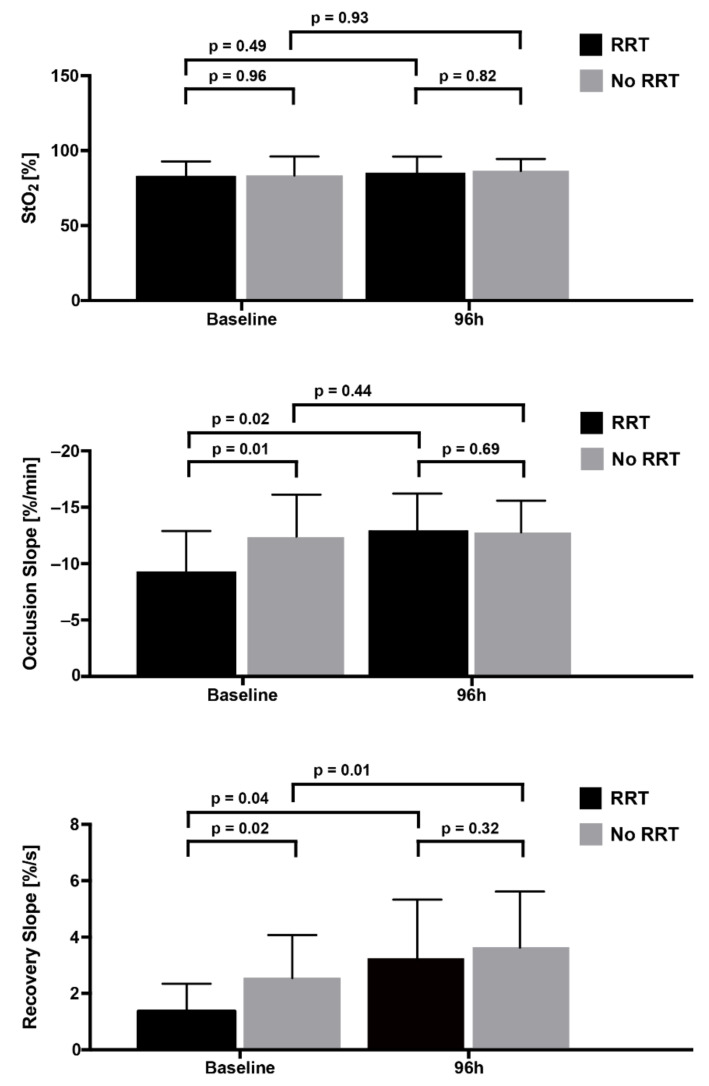
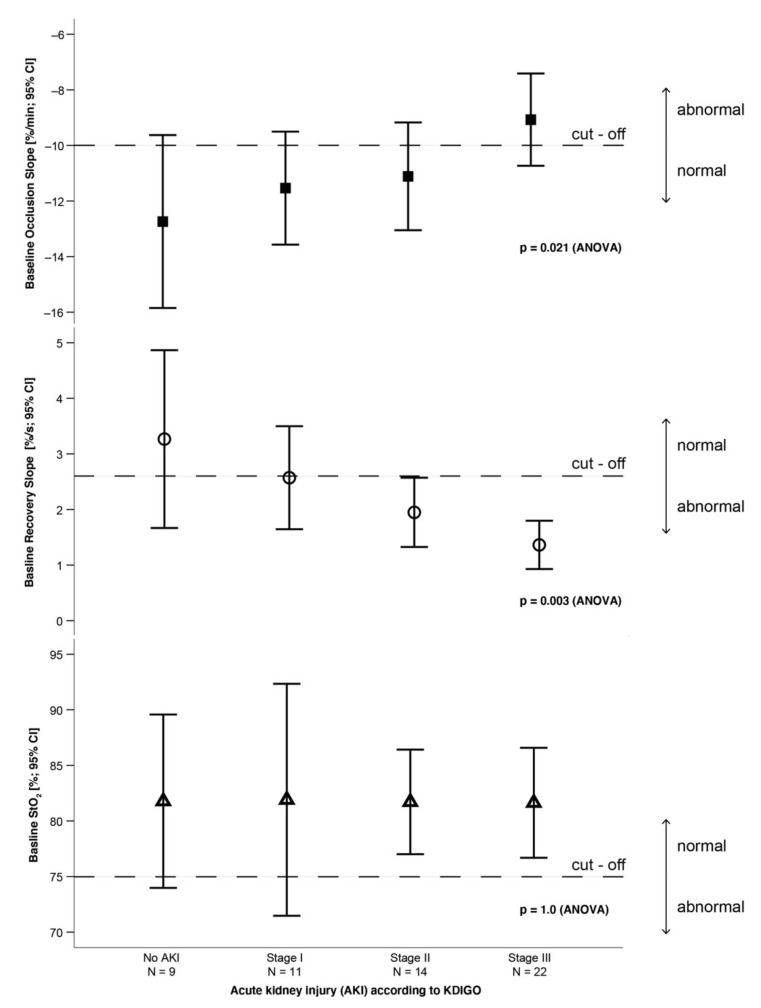
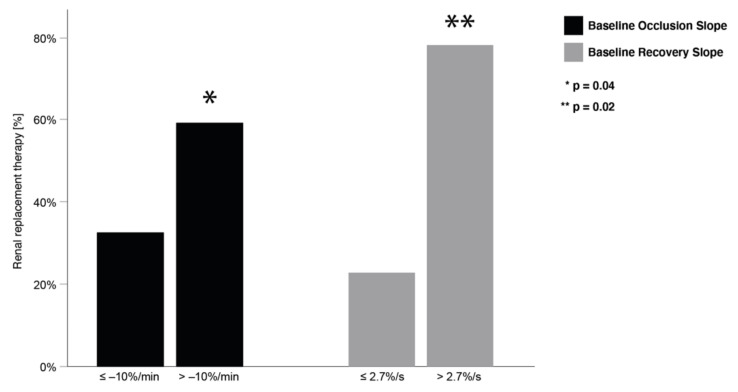
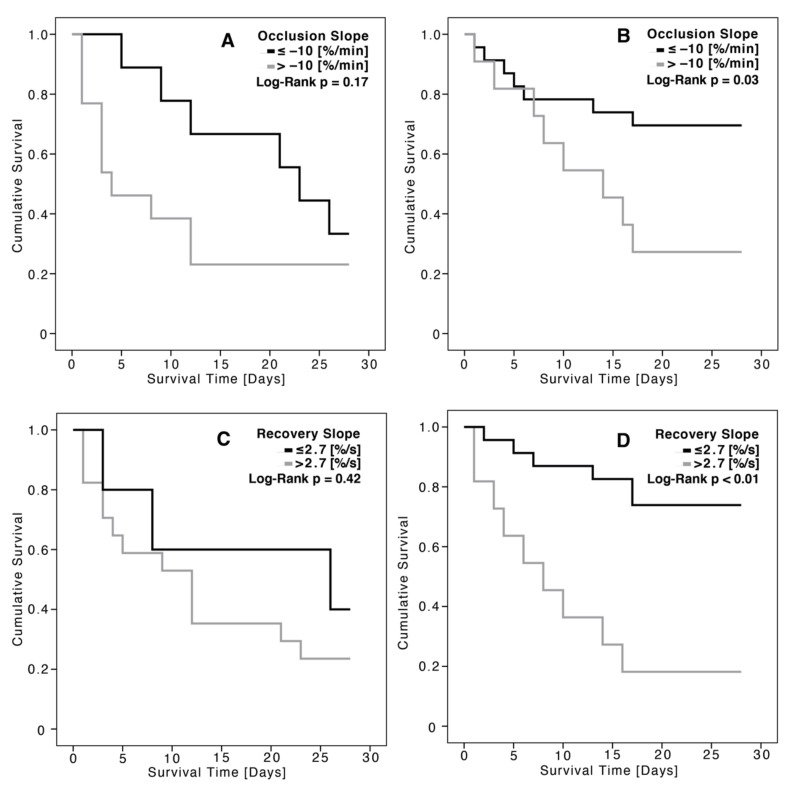
Results: 56 patients with MODS were included in the study (aged 62.5 ± 14.4 years, 40 men and 16 women, APACHE II score 34.5 ± 6.4). Incidences of the different AKI stages were: no AKI, 16.1% (n = 9); AKI stage I, 19.6% (n = 11); AKI stage II, 25% (n = 14); AKI stage III, 39.3% (n = 22). Thus, 39.3% of the patients (n = 22) developed the need for renal replacement therapy (AKI stage III). These patients had a significantly higher mortality over 28 days (RRT, 72% (n = 16/22) vs. no RRT, 44% (n = 15/34); p = 0.03). The mean unprovoked StO2 of all patients at baseline was 81.7 ± 11.1%, and did not differ between patients with or without the need for RRT. Patients with RRT showed significantly weaker negative values of the OS (-9.1 ± 3.7 vs. -11.7 ± 4.1%/min, p = 0.01) and lower values for the RS (1.7 ± 0.9 vs. 2.3 ± 1.6%/s, p = 0.02) compared to non-dialysis patients. Consistent with these results, weaker negative values of the OS were found in higher AKI stages (no AKI, -12.7 ± 4.1%/min; AKI stage I, -11.5 ± 3.0%/min; AKI stage II, -11.1 ± 3.3%/min; AKI stage III, -9.1 ± 3.7%/min; p = 0.021). Unprovoked StO2 did not contain prognostic information regarding the AKI stages.
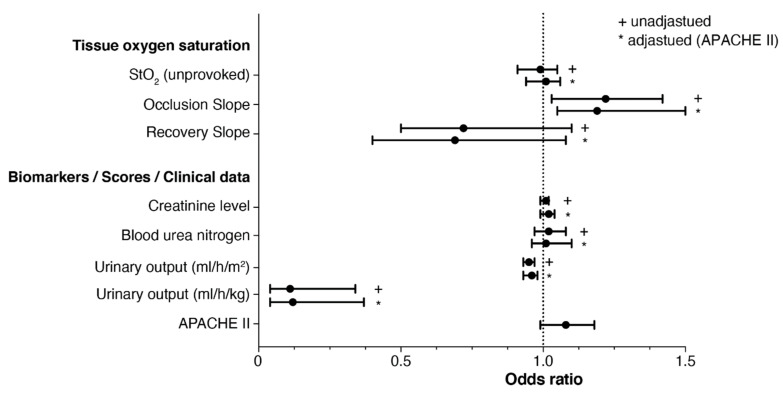
Conclusions: The weaker negative values of the VOT parameter OS are associated with an increased risk of developing AKI and RRT, and increased mortality in the early phase of MODS, while unprovoked StO2 does not contain prognostic information in that regard.
Keywords: MODS; acute kidney injury; intensive care; tissue oxygen saturation.
Conflict of interest statement
We declare no relevant conflict of interest.
Figures
Similar articles
-
Prognostic Value of Tissue Oxygen Saturation Using a Vascular Occlusion Test in Patients in the Early Phase of Multiorgan Dysfunction Syndrome.Shock. 2019 Jun;51(6):706-712. doi: 10.1097/SHK.0000000000001225. Shock. 2019. PMID: 30052575 Clinical Trial.
-
Near-infrared spectroscopy combined with vascular occlusion test to predict acute kidney injury in patients undergoing cardiac surgery: a prospective observational study.J Cardiothorac Surg. 2025 Jan 9;20(1):48. doi: 10.1186/s13019-024-03312-7. J Cardiothorac Surg. 2025. PMID: 39780209 Free PMC article.
-
[Risk factors analysis of renal replacement therapy after liver transplantation and prognosis effect of initial treatment time].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 Nov;30(11):1056-1060. doi: 10.3760/cma.j.issn.2095-4352.2018.011.009. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 30541645 Clinical Trial. Chinese.
-
Timing of renal replacement therapy initiation for acute kidney injury in critically ill patients: a systematic review of randomized clinical trials with meta-analysis and trial sequential analysis.Crit Care. 2021 Jan 6;25(1):15. doi: 10.1186/s13054-020-03451-y. Crit Care. 2021. PMID: 33407756 Free PMC article.
-
Acute kidney injury in burn patients admitted to the intensive care unit: a systematic review and meta-analysis.Crit Care. 2020 Jan 2;24(1):2. doi: 10.1186/s13054-019-2710-4. Crit Care. 2020. PMID: 31898523 Free PMC article.
References
-
- Brivet F.G., Kleinknecht D.J., Loirat P., Landais P.J. Acute renal failure in intensive care units—Causes, outcome, and prognostic factors of hospital mortality; a prospective, multicenter study. French Study Group on Acute Renal Failure. Crit. Care Med. 1996;24:192–198. doi: 10.1097/00003246-199602000-00003. - DOI - PubMed
-
- Hoste E.A., Bagshaw S.M., Bellomo R., Cely C.M., Colman R., Cruz D.N., Edipidis K., Forni L.G., Gomersall C.D., Govil D., et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. doi: 10.1007/s00134-015-3934-7. - DOI - PubMed
LinkOut - more resources
Full Text Sources
