

HIPEC in Peritoneal Metastasis of Gastric Origin: A Systematic Review of Regimens and Techniques
- PMID: 35268546
- PMCID: PMC8911234
- DOI: 10.3390/jcm11051456
HIPEC in Peritoneal Metastasis of Gastric Origin: A Systematic Review of Regimens and Techniques
Abstract
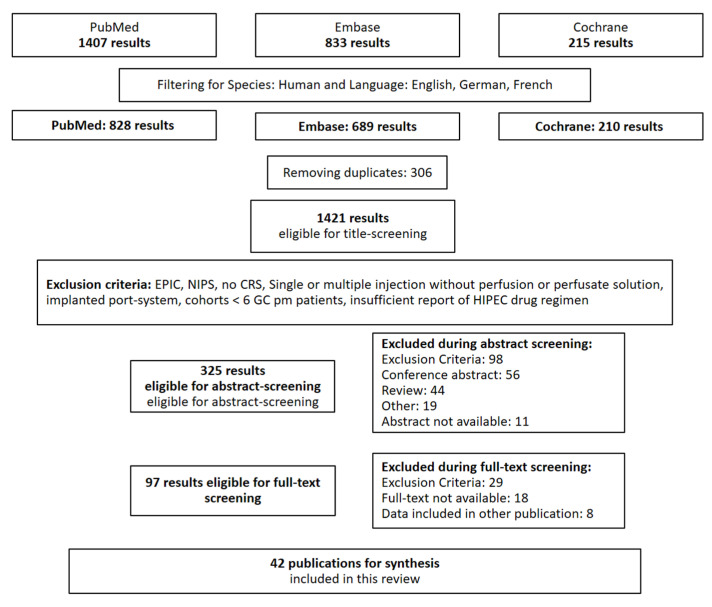
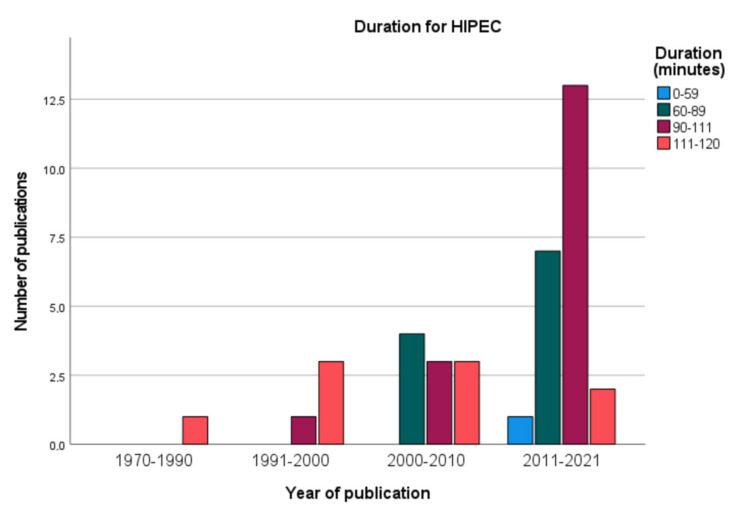
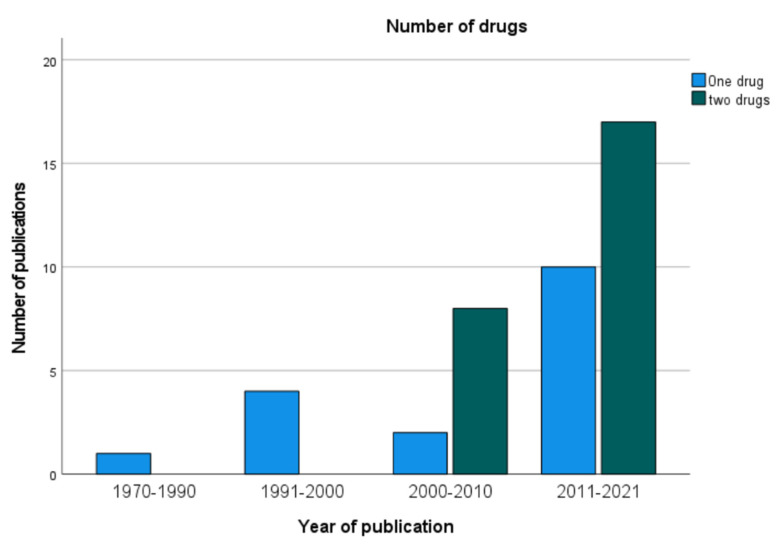
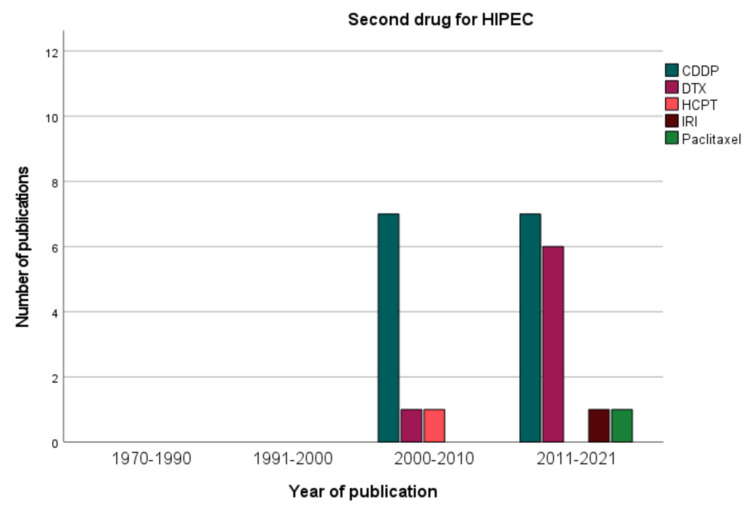
(1) Background: Peritoneal metastasis in gastric cancer is associated with a poor prognosis. Complete cytoreductive surgery including gastrectomy and complete removal of all peritoneal lesions followed by hyperthermic intraperitoneal chemotherapy (HIPEC) achieves promising results. There exists an immersive variety of approaches for HIPEC that makes it difficult to weigh different results obtained in the literature. In order to enable standardization and development of HIPEC, we here present a systematic review of different drug regimens and technical approaches. (2) Methods: PubMed, Embase, and the Cochrane Library were systematically searched on 26 May 2021 using the mesh terms "intraperitoneal chemotherapy AND gastric cancer". Under consideration of systematic review guidelines, articles reporting on HIPEC in combination with CRS were selected. Data on duration, drugs, dosage, and other application parameters as well as morbidity and long term survival data were extracted for subsequent statistical analysis, tabulation, and descriptive synthesis. We assessed the risk of bias due to inhomogeneity of the patient cohort and incompleteness of report of HIPEC parameters. (3) Results: Out of 1421 screened publications, 42 publications presenting data from 1325 patients met the criteria. Most of the publications were single institutional retrospective cohort studies. The most common HIPEC regimen is performed after gastrointestinal anastomosis and consists of 50-200 mg/m2 cisplatinum and 30-40 mg/m2 mytomycin C at 42-43 °C for 60-90 min in a closed abdomen HIPEC system with three tubes. Almost every study reported incompletely on HIPEC parameters. Lower rates of anastomotic leakage were reported in studies that performed HIPEC after gastrointestinal anastomosis. Studies that performed open HIPEC and integrated a two-drug regimen indicated better overall survival rates. (4) Discussion: This is an exhaustive overview of the use of drug regimens and techniques for HIPEC after CRS for gastric cancer peritoneal metastasis. Other indications and application modes of intraperitoneal chemotherapy such as prophylactic or palliative HIPEC apart from CRS were not addressed. (5) Conclusion: Complete report of HIPEC parameters should be included in every publication. A consensus for dose expression either per BSA or as flat dose is desirable for comparison of the drug regimens. Despite numerous variations, we identified the most common regimens and techniques and their advantages and disadvantages according to the data in the literature. More phase I/II studies are needed to identify the best approach for HIPEC. (6) Other: This review was not supported by third parties.
Keywords: PRISMA; cytoreductive surgery; gastric cancer; hyperthermic intraperitoneal chemotherapy (HIPEC); intraperitoneal chemotherapy; peritoneal metastasis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Thomassen I., van Gestel Y.R., van Ramshorst B., Luyer M.D., Bosscha K., Nienhuijs S.W., Lemmens V.E., de Hingh I.H. Peritoneal carcinomatosis of gastric origin: A population-based study on incidence, survival and risk factors. Int. J. Cancer. 2014;134:622–628. doi: 10.1002/ijc.28373. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
