

Long-Term Subjective and Objective Assessment of Smell and Taste in COVID-19
- PMID: 35269410
- PMCID: PMC8909596
- DOI: 10.3390/cells11050788
Long-Term Subjective and Objective Assessment of Smell and Taste in COVID-19
Abstract
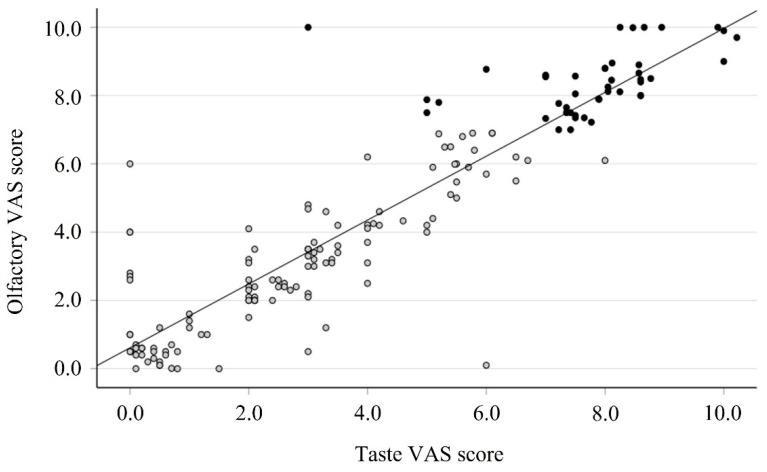
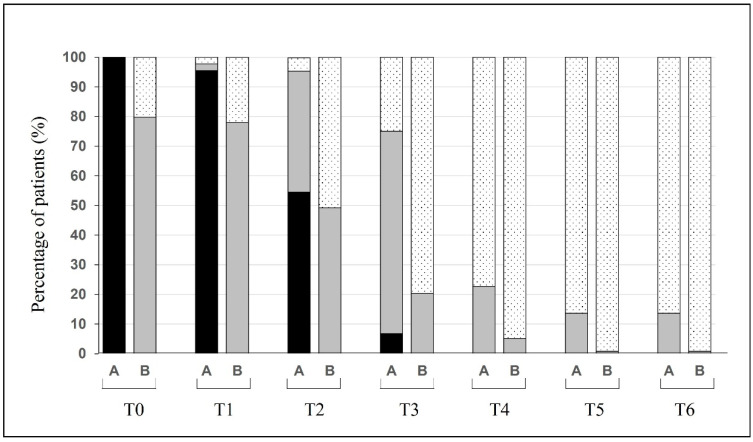
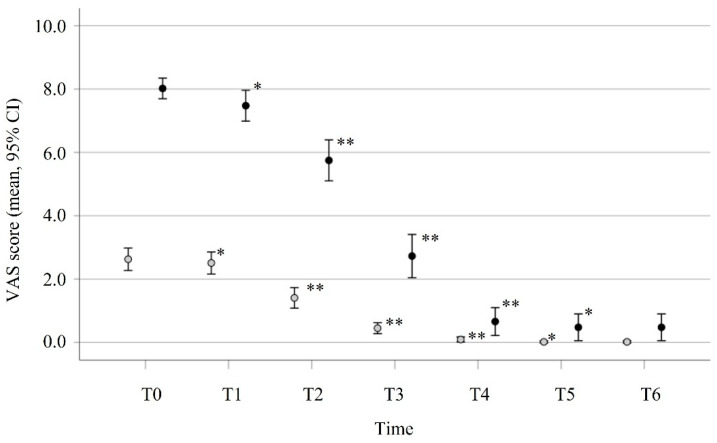
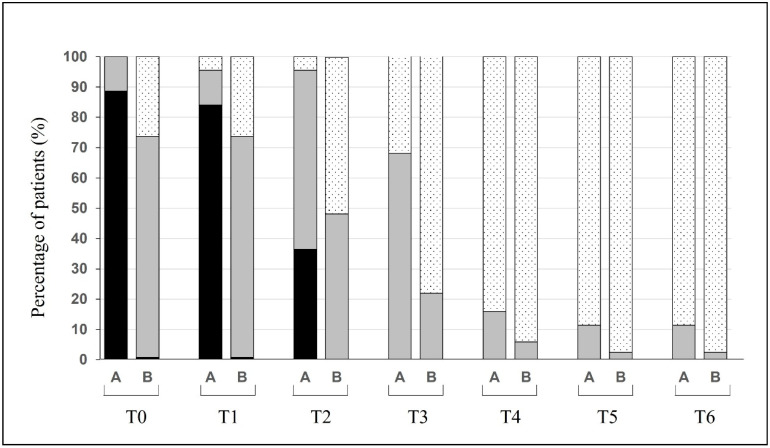
Among the first clinical symptoms of the SARS-CoV-2 infection is olfactory−gustatory deficit; this continues for weeks and, in some cases, can be persistent. We prospectively evaluated 162 patients affected by COVID-19 using a visual analogue scale (VAS) for nasal and olfactory−gustatory symptoms. Patients were checked after 7, 14, 21, 28, 90, and 180 days. A total of 118 patients (72.8%) reported an olfactory VAS < 7 at baseline (group B), and 44 (27.2%) reported anosmia (VAS ≥ 7) (group A) and underwent the Brief Smell Identification Test (B-SIT) and Burghart Taste Strips (BTS) to quantify the deficit objectively and repeated the tests to confirm the sense recovery. Group A patients showed B-SIT anosmia and hyposmia in 44.2% and 55.8% of cases, respectively. A total of 88.6% of group A patients reported ageusia with VAS ≥ 7, and BTS confirmed 81.8% of ageusia and 18.2% of hypogeusia. VAS smell recovery was recorded starting from 14 days, with normalization at 28 days. The 28-day B-SIT score showed normosmia in 90.6% of group A patients. The mean time for full recovery (VAS = 0) was shorter in group B (22.9 days) than in group A (31.9 days). Chemosensory deficit is frequently the first symptom in patients with COVID-19, and, in most cases, recovery occurs after four weeks.
Keywords: B-SIT; COVID-19; smell; taste; taste strips.
Conflict of interest statement
A.C., S.M., A.D.C., I.F., F.L.R., S.B., E.B., A.A., A.C., I.M., C.M.M., M.d.V., A.G., L.Z. and M.A. declare no conflict of interest. C.C. declares scientific consultancy for GlaxoSmithKline.
Figures
References
-
- World Health Organization WHO Coronavirus (COVID-19) Dashboard. [(accessed on 18 December 2021)]. Available online: https://covid19.who.int/
-
- Lechien J.R., Chiesa-Estomba C.M., Vaira L.A., De Riu G., Cammaroto G., Chekkoury-Idrissi Y., Circiu M., Distinguin L., Journe F., de Terwangne C., et al. Epidemiological, otolaryngological, olfactory and gustatory outcomes according to the severity of COVID-19: A study of 2579 patients. Eur. Arch. Otorhinolaryngol. 2021;278:2851–2859. doi: 10.1007/s00405-020-06548-w. - DOI - PMC - PubMed
-
- Nakagawara K., Masaki K., Uwamino Y., Kabata H., Uchida S., Uno S., Asakura T., Funakoshi T., Kanzaki S., Ishii M., et al. Acute onset olfactory/taste disorders are associated with a high viral burden in mild or asymptomatic SARS-CoV-2 infections. Int. J. Infect. Dis. 2020;99:19–22. doi: 10.1016/j.ijid.2020.07.034. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
