

Sarcopenic Obesity Tendency and Nutritional Status Is Related to the Risk of Sarcopenia, Frailty, Depression and Quality of Life in Patients with Dementia
- PMID: 35270185
- PMCID: PMC8908993
- DOI: 10.3390/ijerph19052492
Sarcopenic Obesity Tendency and Nutritional Status Is Related to the Risk of Sarcopenia, Frailty, Depression and Quality of Life in Patients with Dementia
Abstract
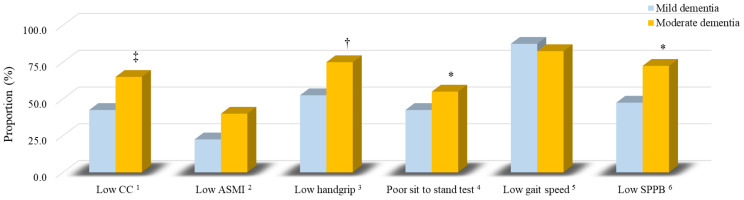
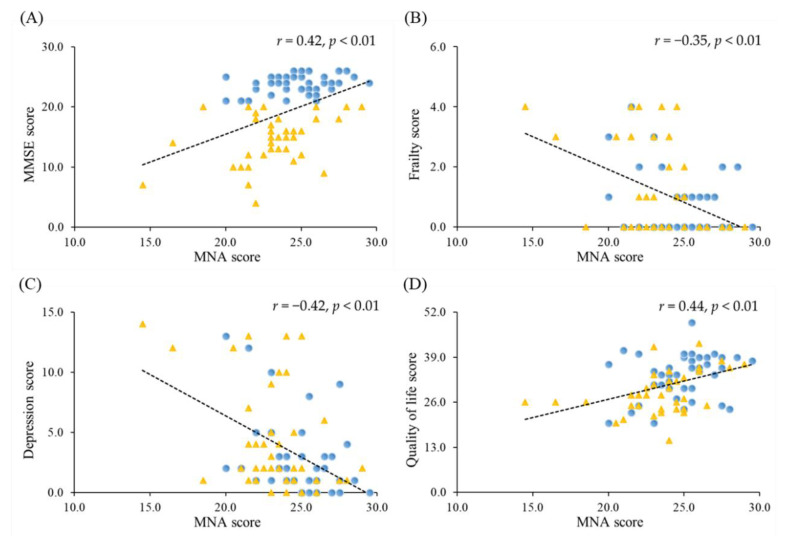
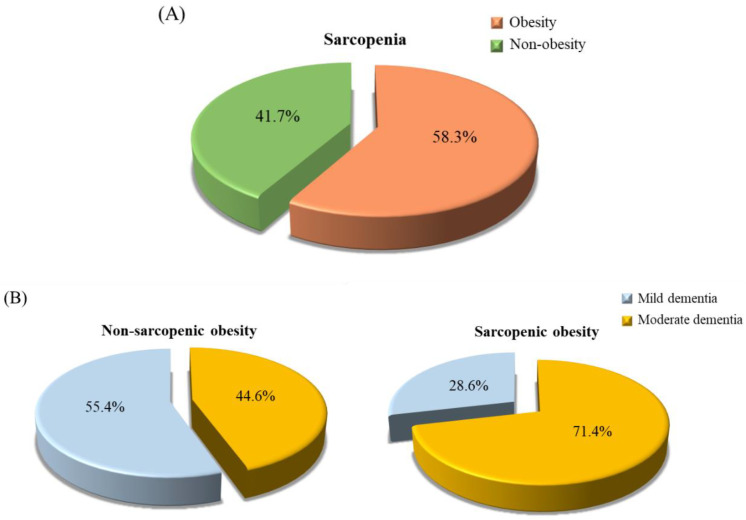
The purpose of this study was to investigate the nutritional status of dementia patients and examine the correlation with sarcopenia, frailty, depression, and quality of life. We enrolled patients aged 60 years and over with Mini Mental State Examination (MMSE) scores ≤ 26 (Taiwan), and dementia diagnosed by a neurologist or psychiatrist. Nutritional status was assessed with the Mini Nutritional Assessment (MNA). Muscle mass was measured by dual-energy X-ray absorptiometry. Muscle strength and endurance were evaluated by handgrip, leg-back strength, dumbbell curls, sit to stand test, and gait speed. Quality of life, frailty, and depression status were measured by questionnaires. Patients with moderate dementia (MMSE ≤ 20) had a significantly lower MNA score, muscle function, and quality of life than patients with mild dementia (p < 0.01). A lower MNA score was significantly associated with the risk of frailty (odds ratio: 4.76, p < 0.01), depression (odds ratio: 3.17, p = 0.03), and poor quality of life (odds ratio: 2.73, p < 0.05), and sarcopenia (odds ratio: 3.97, p = 0.03) after adjusting for potential confounders. In conclusion, patients with dementia were at risk of malnutrition, and nutritional status was associated to the risk of sarcopenia, frailty, depression, and quality of life.
Keywords: dementia; depression; frailty; nutritional status; quality of life; sarcopenia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization The Top 10 Causes of Death. [(accessed on 12 August 2021)]. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
-
- Taiwan Alzheimer Disease Association People with Dementia in Taiwan. (April 2021) [(accessed on 7 February 2022)]. Available online: http://www.tada2002.org.tw/About/IsntDementia#bn1.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
