

Challenges in Diagnosis and Prevention of Iatrogenic Endometriosis as a Long-Term Surgical Complication after C-Section
- PMID: 35270482
- PMCID: PMC8910041
- DOI: 10.3390/ijerph19052791
Challenges in Diagnosis and Prevention of Iatrogenic Endometriosis as a Long-Term Surgical Complication after C-Section
Abstract
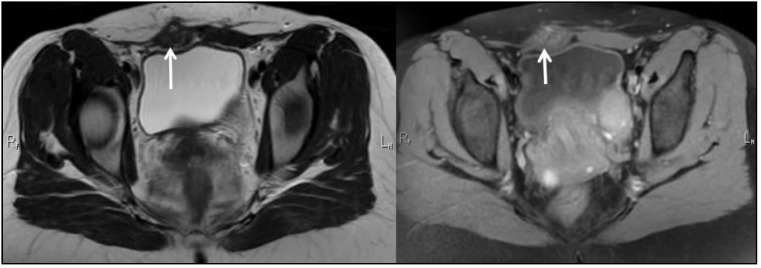
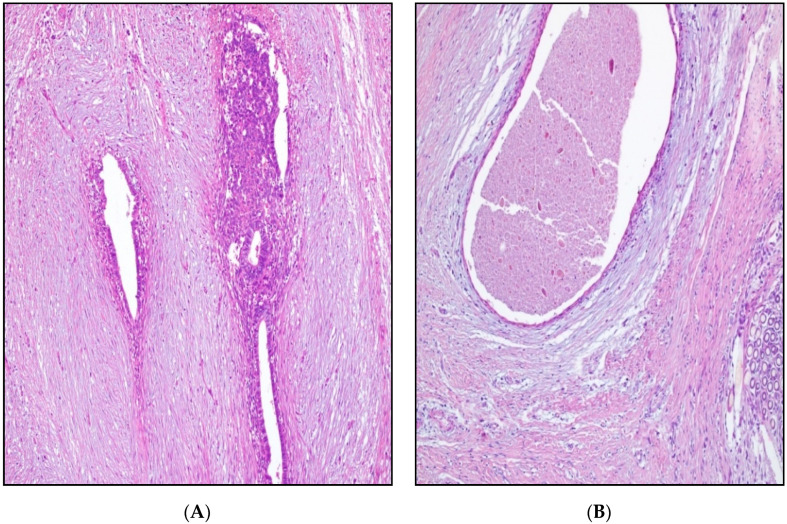
Endometriosis is a gynecological condition caused by the development of endometrial tissue outside the uterine cavity. Naturally, it commonly occurs at locations such as the ovaries and pelvic peritoneum. However, ectopic endometrial tissue may be discovered outside of the typical sites, suggesting the possibility of iatrogenic seeding after gynecological operations. Based on this hypothesis, we developed a study aiming to establish the root cause of atypical implantation of endometrial foci, as the main end point, and to determine diagnostic features and risk factors for this condition, as a secondary target. The research followed a retrospective design, including a total of 126 patients with endometriosis who met the inclusion criteria. A group of 71 patients with a history of c-section was compared with a control group of patients with endometriosis and no history of c-section. Endometriosis that developed inside or in close proximity to surgical incisions of asymptomatic patients before surgical intervention was defined as iatrogenic endometriosis. Compared with patients who did not have a c-section, the c-section group had significantly more minimally invasive pelvic procedures and multiple adhesions and endometriosis foci at intraoperative look (52.1% vs. 34.5%, respectively 52.1% vs. 29.1%). The most common location for endometriosis lesions in patients with prior c-section was the abdominal wall (42.2% vs. 5.4%), although the size of foci was significantly smaller by size and weight (32.2 mm vs. 34.8 mm, respectively 48.6 g vs. 53.1 g). The abdominal wall endometriosis was significantly associated with minimally invasive pelvic procedures (correlation coefficient = 0.469, p-value = 0.001) and c-section (correlation coefficient = 0.523, p-value = 0.001). A multivariate regression analysis identified prior c-section as an independent risk factor for abdominal wall endometriosis (OR = 1.85, p-value < 0.001). We advocate for strict protocols to be implemented and followed during c-section and minimally invasive procedures involving the pelvic region to ensure minimum spillage of endometrial cells. Further research should be developed to determine the method of abdominal and surgical site irrigation that can significantly reduce the risk of implantation of viable endometrial cells. Understanding all details of iatrogenic endometriosis will lead to the development of non-invasive disease diagnosis and minimally invasive procedures that have the potential to reduce postoperative complications.
Keywords: amniotic fluid; cesarean section; endometriosis; iatrogenic disease; surgical scars.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Hudelist G., Ballard K., English J., Wright J., Banerjee S., Mastoroudes H., Thomas A., Singer C.F., Keckstein J. Transvaginal sonography vs. clinical examination in the preoperative diagnosis of deep infiltrating endometriosis. Ultrasound Obstet. Gynecol. 2011;37:480–487. doi: 10.1002/uog.8935. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
