

A clinical observational analysis of aerosol emissions from dental procedures
- PMID: 35271682
- PMCID: PMC8912243
- DOI: 10.1371/journal.pone.0265076
A clinical observational analysis of aerosol emissions from dental procedures
Abstract
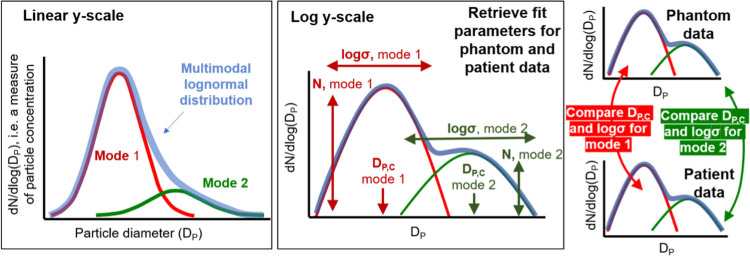
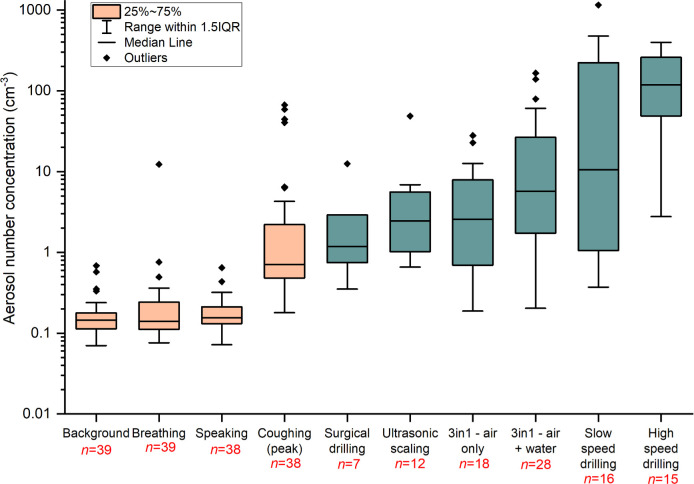
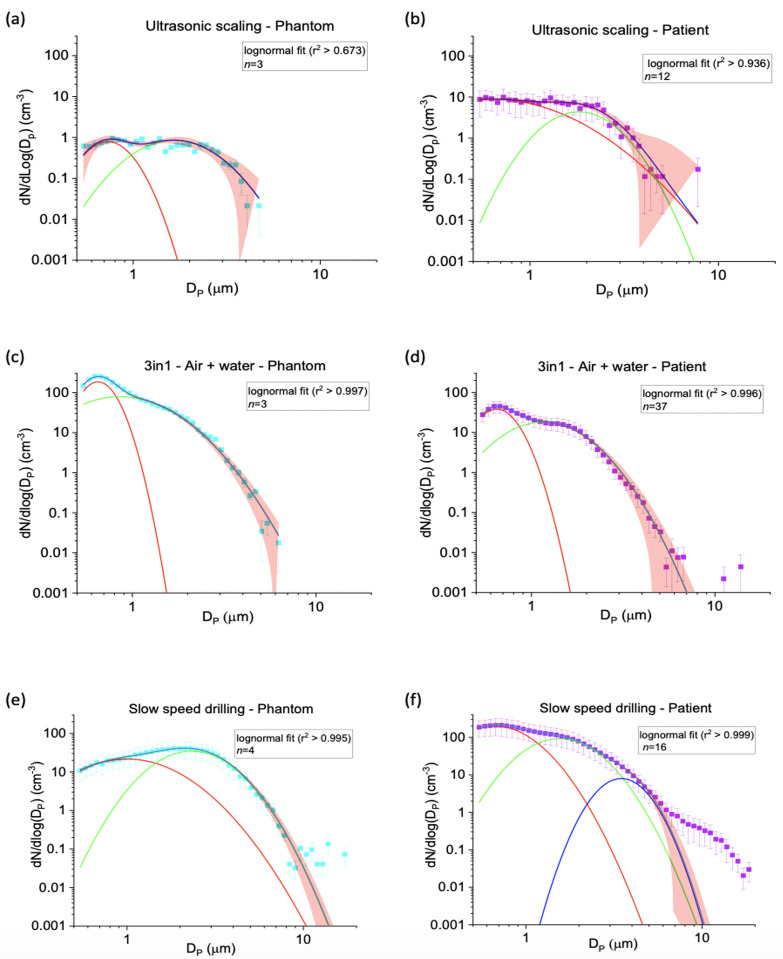
Aerosol generating procedures (AGPs) are defined as any procedure releasing airborne particles <5 μm in size from the respiratory tract. There remains uncertainty about which dental procedures constitute AGPs. We quantified the aerosol number concentration generated during a range of periodontal, oral surgery and orthodontic procedures using an aerodynamic particle sizer, which measures aerosol number concentrations and size distribution across the 0.5-20 μm diameter size range. Measurements were conducted in an environment with a sufficiently low background to detect a patient's cough, enabling confident identification of aerosol. Phantom head control experiments for each procedure were performed under the same conditions as a comparison. Where aerosol was detected during a patient procedure, we assessed whether the size distribution could be explained by the non-salivary contaminated instrument source in the respective phantom head control procedure using a two-sided unpaired t-test (comparing the mode widths (log(σ)) and peak positions (DP,C)). The aerosol size distribution provided a robust fingerprint of aerosol emission from a source. 41 patients underwent fifteen different dental procedures. For nine procedures, no aerosol was detected above background. Where aerosol was detected, the percentage of procedure time that aerosol was observed above background ranged from 12.7% for ultrasonic scaling, to 42.9% for 3-in-1 air + water syringe. For ultrasonic scaling, 3-in-1 syringe use and surgical drilling, the aerosol size distribution matched the non-salivary contaminated instrument source, with no unexplained aerosol. High and slow speed drilling produced aerosol from patient procedures with different size distributions to those measured from the phantom head controls (mode widths log(σ)) and peaks (DP,C, p< 0.002) and, therefore, may pose a greater risk of salivary contamination. This study provides evidence for sources of aerosol generation during common dental procedures, enabling more informed evaluation of risk and appropriate mitigation strategies.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. World Health Organization. Infection prevention and control during health care when novel coronavirus (nCoV) infection is suspected 2020. [Available from: https://www.who.int/publications/i/item/10665-331495.
-
- Jeong HW, Kim S-M, Kim H-S, Kim Y-I, Kim JH, Cho JY, et al.. Viable SARS-CoV-2 in various specimens from COVID-19 patients. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2020;26:1520–4. doi: 10.1016/j.cmi.2020.07.020 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
