

Impact of history of mental disorders on short-term mortality among hospitalized patients with sepsis: A population-based cohort study
- PMID: 35271683
- PMCID: PMC8912146
- DOI: 10.1371/journal.pone.0265240
Impact of history of mental disorders on short-term mortality among hospitalized patients with sepsis: A population-based cohort study
Abstract
Background: Mental disorders are associated with markedly reduced life expectancy, in part due to an increased risk of death due to infection, likely reflecting sepsis-associated mortality. Patients with mental disorders are at an increased risk of sepsis, but data on the prognostic impact of mental disorders in sepsis are sparse, showing conflicting findings.
Methods: We used statewide data to identify hospitalizations aged ≥18 years with sepsis in Texas during 2014-2017. Mental disorders, including mood, anxiety, psychosis, and personality disorders were identified using Clinical Classification Software codes. Multilevel, multivariable logistic regression with propensity adjustment (primary model), with propensity score matching, and multivariable logistic regression as alternative models, were used to estimate the association between mental disorders and short-term mortality (defined as in-hospital mortality or discharge to hospice). Additional models were fitted for sensitivity analyses and to estimate the prognostic associations of individual categories of mental disorders.
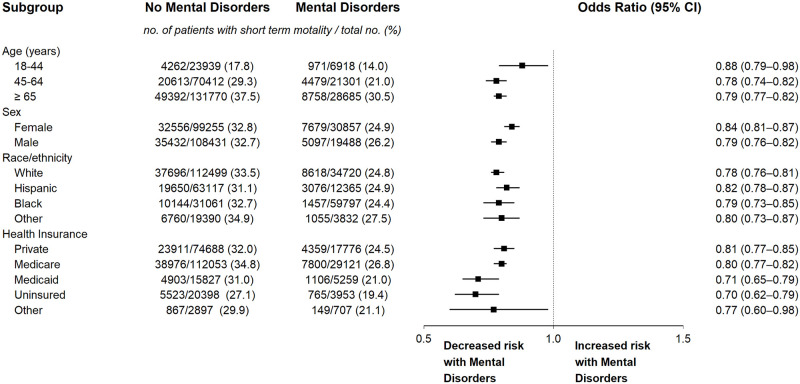
Results: Among 283,025 hospitalizations with sepsis, 56,904 (20.1%) had mental disorders. Hospitalizations with vs without mental disorders were younger (age 18-44 years 12.2% vs 10.6%), more commonly white (61.0% vs 49.8%), with lower burden of comorbidities (mean [SD] Deyo comorbidity index 2.53 [2.27] vs 2.73 [2.47]), and with lower need for organ support (mechanical ventilation 32.8% vs 36.0%); p<0.0001 for all comparisons. Crude short-term mortality among sepsis hospitalizations with and without mental disorders was 25.0% vs 32.8%, respectively. On adjusted analyses, mental disorders remained associated with lower odds of short-term mortality (adjusted odds ratio 0.792 [95% CI 0.772-0.812]). This finding was consistent on the alternative modeling approaches, sensitivity analyses, and examination of individual categories of mental disorders.
Conclusions: Mental disorders were associated, unexpectedly, with markedly lower risk of short-term mortality in sepsis. Further studies to examine the mechanisms underlying these findings may inform future efforts to improve sepsis outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The association of systemic lupus erythematosus with short-term mortality in sepsis: a population-level analysis.J Investig Med. 2023 Apr;71(4):419-428. doi: 10.1177/10815589221150641. Epub 2023 Jan 19. J Investig Med. 2023. PMID: 36655787
-
The prognostic impact of rheumatoid arthritis in sepsis: a population-based analysis.Acute Crit Care. 2022 Nov;37(4):533-542. doi: 10.4266/acc.2022.00787. Epub 2022 Oct 6. Acute Crit Care. 2022. PMID: 36203231 Free PMC article.
-
Previously healthy adults among septic patients: Population-level epidemiology and outcomes.J Crit Care. 2024 Feb;79:154427. doi: 10.1016/j.jcrc.2023.154427. Epub 2023 Sep 15. J Crit Care. 2024. PMID: 37717361
-
Association of multiple sclerosis with mortality in sepsis: a population-level analysis.J Intensive Care. 2022 Jul 25;10(1):36. doi: 10.1186/s40560-022-00628-1. J Intensive Care. 2022. PMID: 35879778 Free PMC article.
-
Long term mortality in critically ill burn survivors.Burns. 2017 Sep;43(6):1155-1162. doi: 10.1016/j.burns.2017.05.010. Epub 2017 Jun 9. Burns. 2017. PMID: 28606748
Cited by
-
Association of severe mental illness and septic shock case fatality rate in patients admitted to the intensive care unit: A national population-based cohort study.PLoS Med. 2023 Mar 13;20(3):e1004202. doi: 10.1371/journal.pmed.1004202. eCollection 2023 Mar. PLoS Med. 2023. PMID: 36913434 Free PMC article.
-
The effects of sociodemographic factors and comorbidities on sepsis: A nationwide Swedish cohort study.Prev Med Rep. 2023 Jul 16;35:102326. doi: 10.1016/j.pmedr.2023.102326. eCollection 2023 Oct. Prev Med Rep. 2023. PMID: 37519448 Free PMC article.
-
Severe mental illness and mortality in sepsis and septic shock: a systematic review and meta-analysis.Mol Psychiatry. 2024 Dec;29(12):3857-3864. doi: 10.1038/s41380-024-02603-8. Epub 2024 May 20. Mol Psychiatry. 2024. PMID: 38769373
-
Severe mental illness and infectious disease mortality: a systematic review and meta-analysis.EClinicalMedicine. 2024 Oct 9;77:102867. doi: 10.1016/j.eclinm.2024.102867. eCollection 2024 Nov. EClinicalMedicine. 2024. PMID: 39649134 Free PMC article.
-
Causal associations between severe mental illness and sepsis: a Mendelian randomization study.Front Psychiatry. 2024 Mar 12;15:1341559. doi: 10.3389/fpsyt.2024.1341559. eCollection 2024. Front Psychiatry. 2024. PMID: 38532990 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
