

International expert consensus recommendations for the diagnosis and treatment of Langerhans cell histiocytosis in adults
- PMID: 35271698
- PMCID: PMC11022927
- DOI: 10.1182/blood.2021014343
International expert consensus recommendations for the diagnosis and treatment of Langerhans cell histiocytosis in adults
Abstract
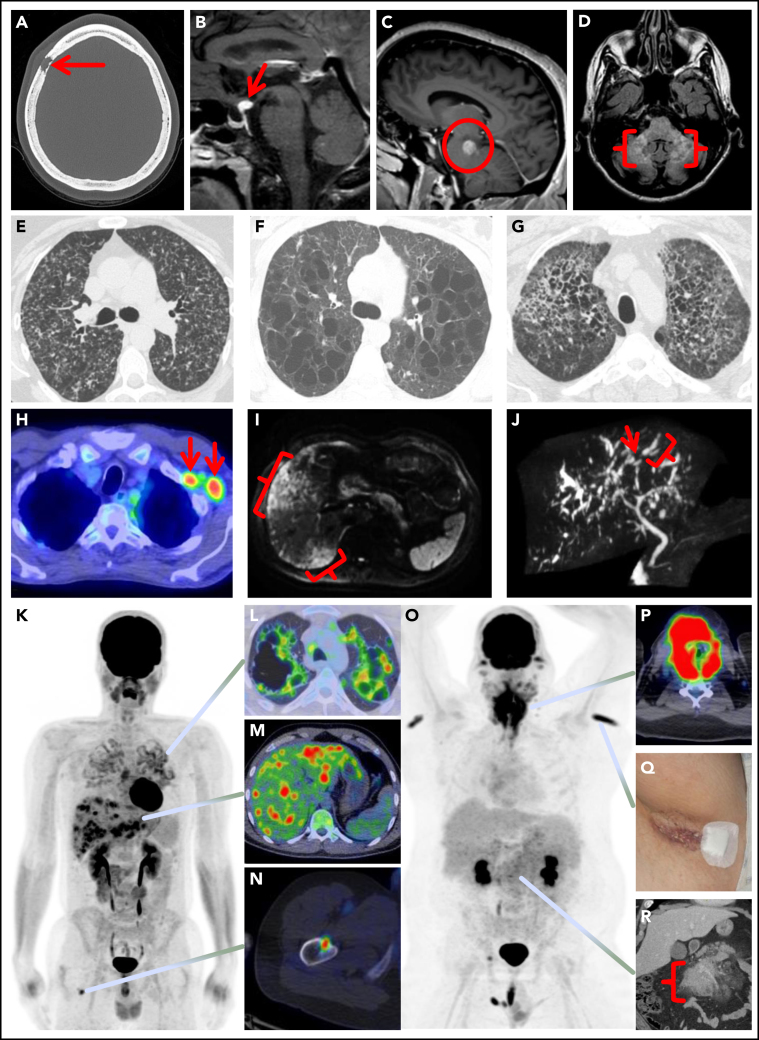
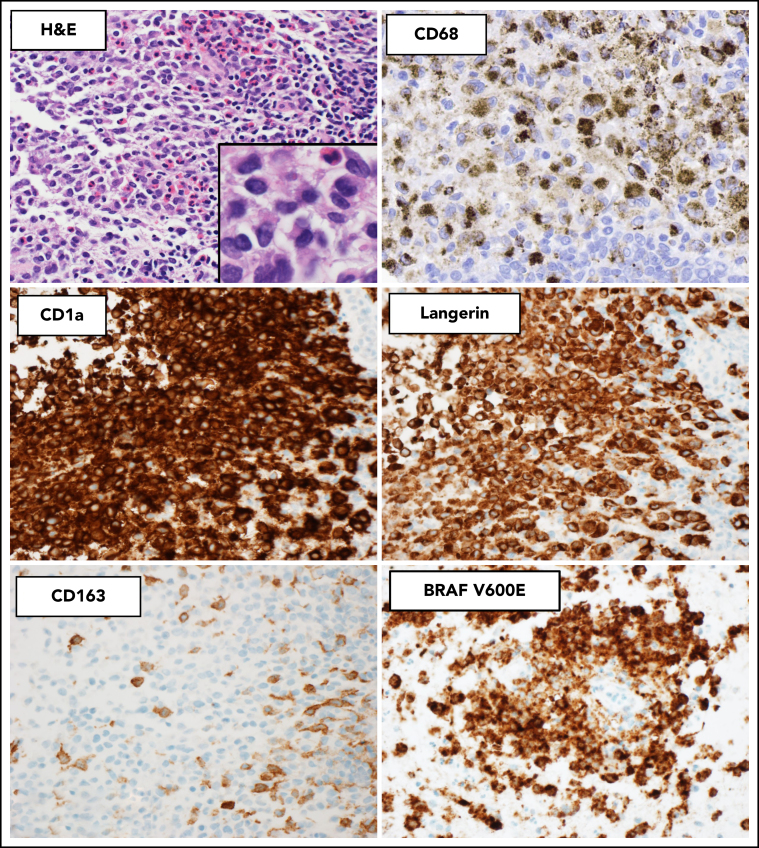
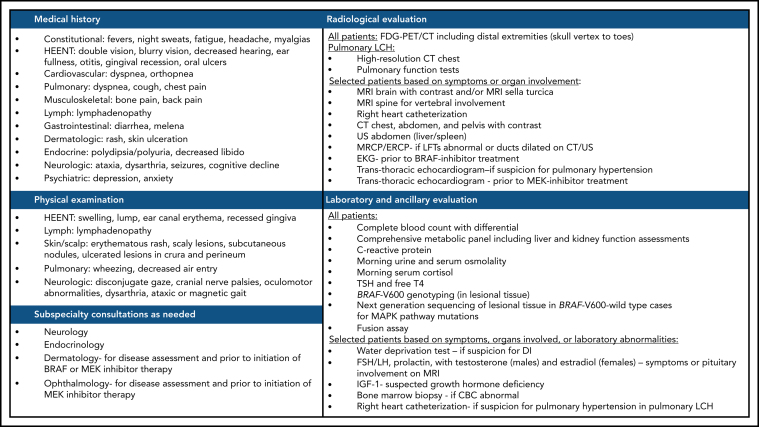
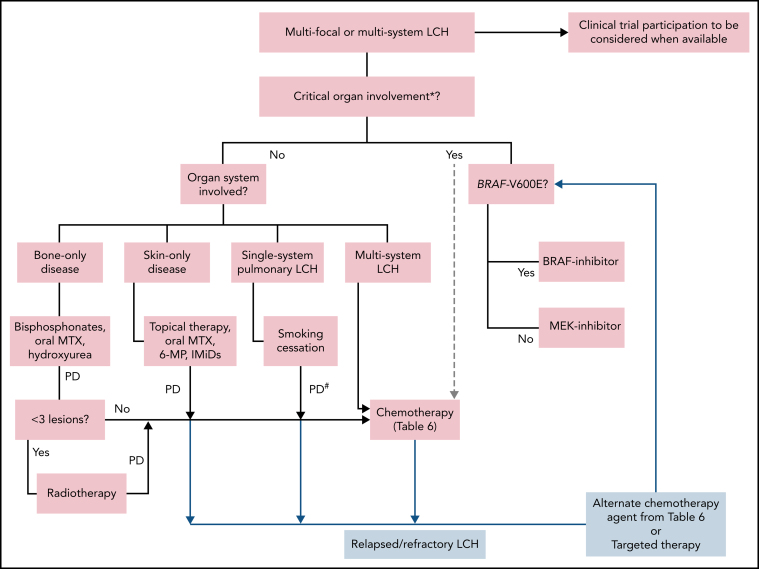
Langerhans cell histiocytosis (LCH) can affect children and adults with a wide variety of clinical manifestations, including unifocal, single-system multifocal, single-system pulmonary (smoking-associated), or multisystem disease. The existing paradigms in the management of LCH in adults are mostly derived from the pediatric literature. Over the last decade, the discovery of clonality and MAPK-ERK pathway mutations in most cases led to the recognition of LCH as a hematopoietic neoplasm, opening the doors for treatment with targeted therapies. These advances have necessitated an update of the existing recommendations for the diagnosis and treatment of LCH in adults. This document presents consensus recommendations that resulted from the discussions at the annual Histiocyte Society meeting in 2019, encompassing clinical features, classification, diagnostic criteria, treatment algorithm, and response assessment for adults with LCH. The recommendations favor the use of 18F-Fluorodeoxyglucose positron emission tomography-based imaging for staging and response assessment in the majority of cases. Most adults with unifocal disease may be cured by local therapies, while the first-line treatment for single-system pulmonary LCH remains smoking cessation. Among patients not amenable or unresponsive to these treatments and/or have multifocal and multisystem disease, systemic treatments are recommended. Preferred systemic treatments in adults with LCH include cladribine or cytarabine, with the emerging role of targeted (BRAF and MEK inhibitor) therapies. Despite documented responses to treatments, many patients struggle with a high symptom burden from pain, fatigue, and mood disorders that should be acknowledged and managed appropriately.
© 2022 by The American Society of Hematology.
Figures
References
-
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. International Agency for Research on Cancer; Lyon, France: 2017.
-
- Goyal G, Shah MV, Hook CC, et al. Adult disseminated Langerhans cell histiocytosis: incidence, racial disparities and long-term outcomes. Br J Haematol. 2018;182(4):579–581. - PubMed
-
- Makras P, Stathi D, Yavropoulou M, Tsoli M, Kaltsas G. The annual incidence of Langerhans cell histiocytosis among adults living in Greece. Pediatr Blood Cancer. 2020;67(9):e28422. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
