

A recipe for a good clinical pulmonary surfactant
- PMID: 35272060
- PMCID: PMC9486245
- DOI: 10.1016/j.bj.2022.03.001
A recipe for a good clinical pulmonary surfactant
Abstract
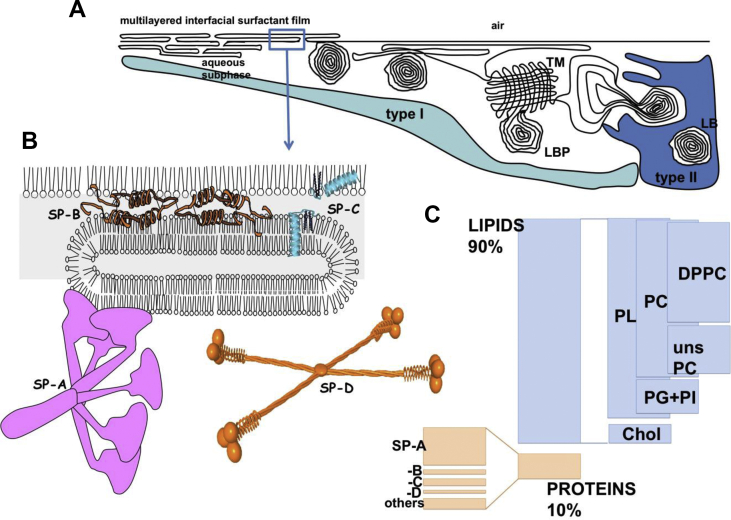
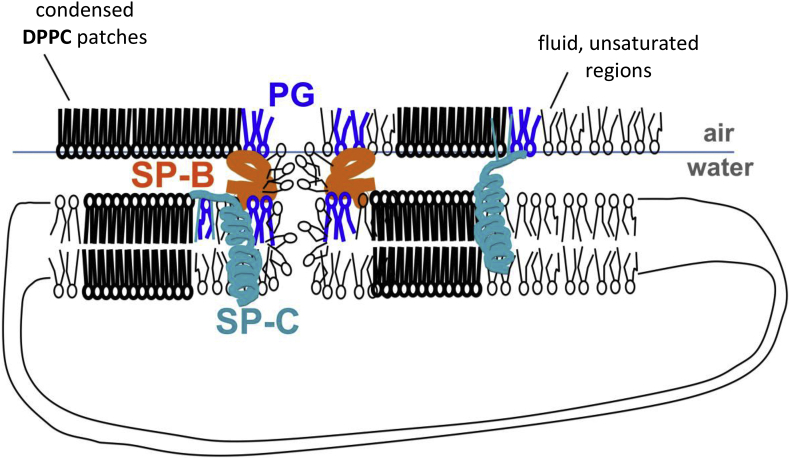
The lives of thousands premature babies have been saved along the last thirty years thanks to the establishment and consolidation of pulmonary surfactant replacement therapies (SRT). It took some time to close the gap between the identification of the biophysical and molecular causes of the high mortality associated with respiratory distress syndrome in very premature babies and the development of a proper therapy. Closing the gap required the elucidation of some key questions defining the structure-function relationships in surfactant as well as the particular role of the different molecular components assembled into the surfactant system. On the other hand, the application of SRT as part of treatments targeting other devastating respiratory pathologies, in babies and adults, is depending on further extensive research still required before enough amounts of good humanized clinical surfactants will be available. This review summarizes our current concepts on the compositional and structural determinants defining pulmonary surfactant activity, the principles behind the development of efficient natural animal-derived or recombinant or synthetic therapeutic surfactants, as well as a the most promising lines of research that are already opening new perspectives in the application of tailored surfactant therapies to treat important yet unresolved respiratory pathologies.
Keywords: ARDS; Air–liquid interface; DPPC; Lipid–protein interactions; Respiratory distress syndrome; Surfactant replacement therapy.
Copyright © 2022 Chang Gung University. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflicts of interest The author has received research grants from Chiesi Farmaceutici SpA, and Airway Therapeutics Inc. He served as lecturer for Chiesi Farmaceutici SpA. He has also been member of advisory boards for Chiesi Farmaceutici SpA and Airway Therapeutics. These companies produce clinical surfactants and/or surfactant proteins or related products, but have not participated in the preparation, review, or approval of the manuscript or in the decision to submit it for publication.
Figures
References
-
- Curstedt T., Halliday H.L., Speer C.P. A unique story in neonatal research: the development of a porcine surfactant. Neonatology. 2015;107:321–329. - PubMed
-
- Speer C.P., Sweet D.G., Halliday H.L. Surfactant therapy: past, present and future. Early Hum Dev. 2013;89(Suppl 1):S22–S24. - PubMed
-
- Castillo-Sanchez J.C., Cruz A., Perez-Gil J. Structural hallmarks of lung surfactant: lipid-protein interactions, membrane structure and future challenges. Arch Biochem Biophys. 2021;703:108850. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
