

Precision measurement of cardiac structure and function in cardiovascular magnetic resonance using machine learning
- PMID: 35272664
- PMCID: PMC8908603
- DOI: 10.1186/s12968-022-00846-4
Precision measurement of cardiac structure and function in cardiovascular magnetic resonance using machine learning
Abstract
Background: Measurement of cardiac structure and function from images (e.g. volumes, mass and derived parameters such as left ventricular (LV) ejection fraction [LVEF]) guides care for millions. This is best assessed using cardiovascular magnetic resonance (CMR), but image analysis is currently performed by individual clinicians, which introduces error. We sought to develop a machine learning algorithm for volumetric analysis of CMR images with demonstrably better precision than human analysis.
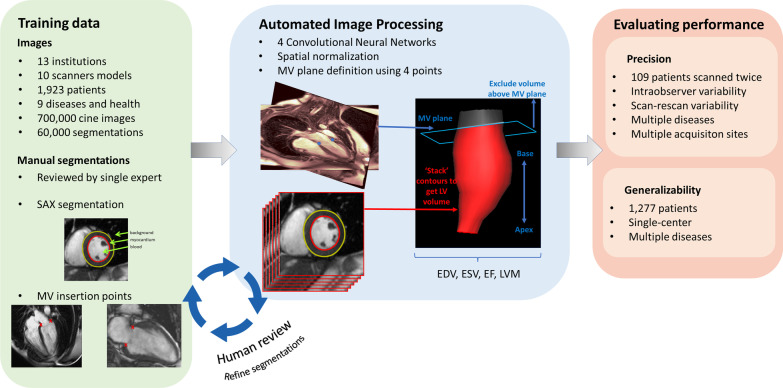
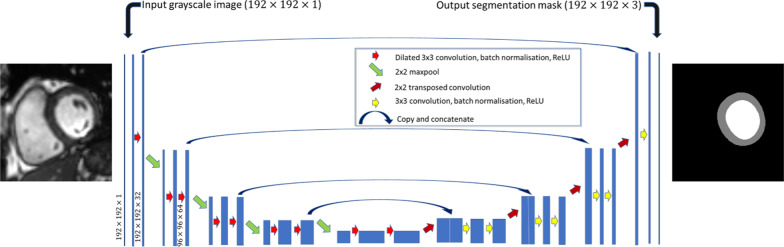
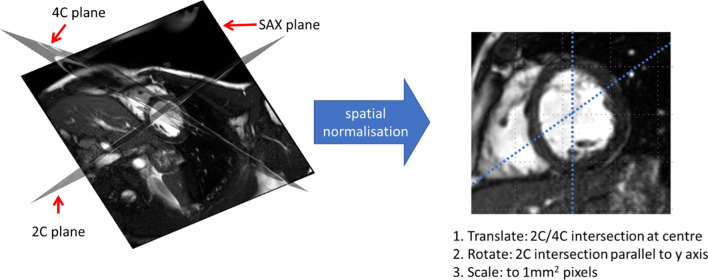
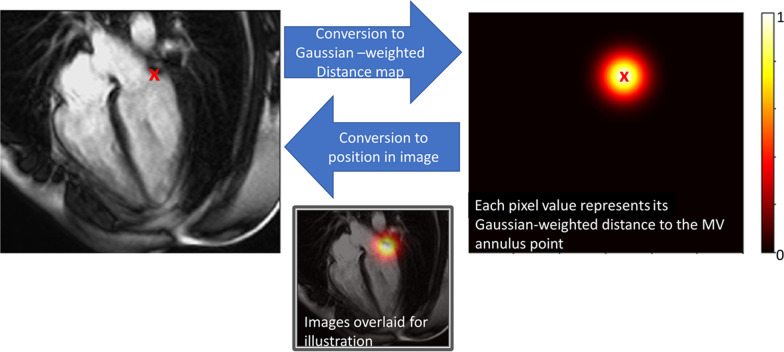
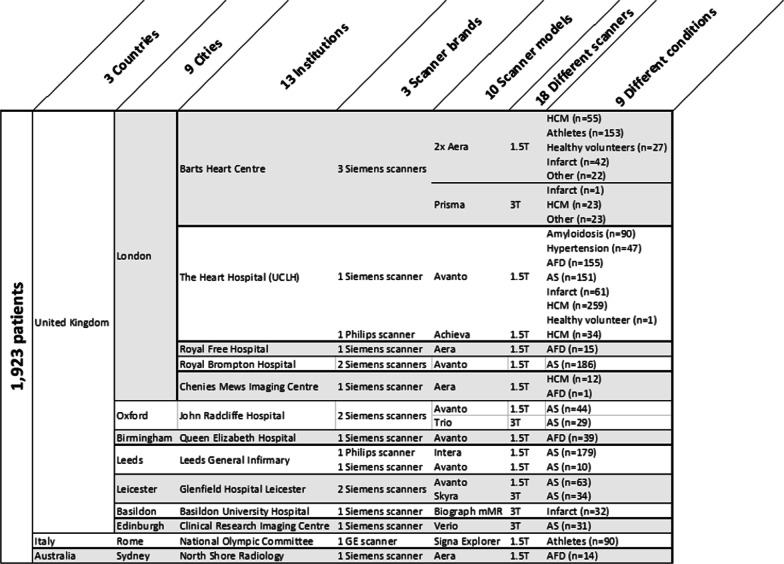
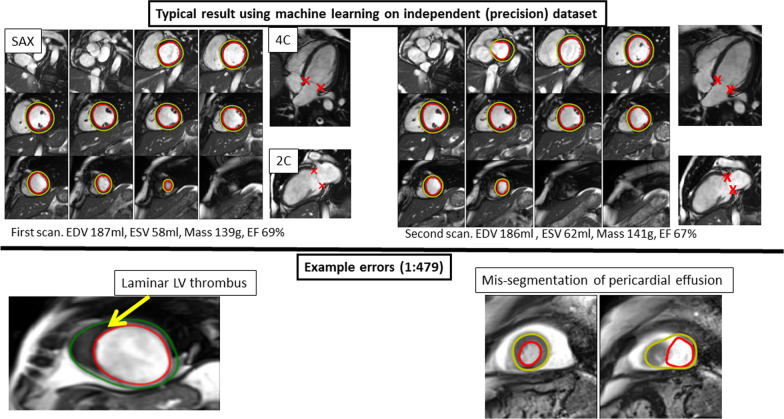
Methods: A fully automated machine learning algorithm was trained on 1923 scans (10 scanner models, 13 institutions, 9 clinical conditions, 60,000 contours) and used to segment the LV blood volume and myocardium. Performance was quantified by measuring precision on an independent multi-site validation dataset with multiple pathologies with n = 109 patients, scanned twice. This dataset was augmented with a further 1277 patients scanned as part of routine clinical care to allow qualitative assessment of generalization ability by identifying mis-segmentations. Machine learning algorithm ('machine') performance was compared to three clinicians ('human') and a commercial tool (cvi42, Circle Cardiovascular Imaging).
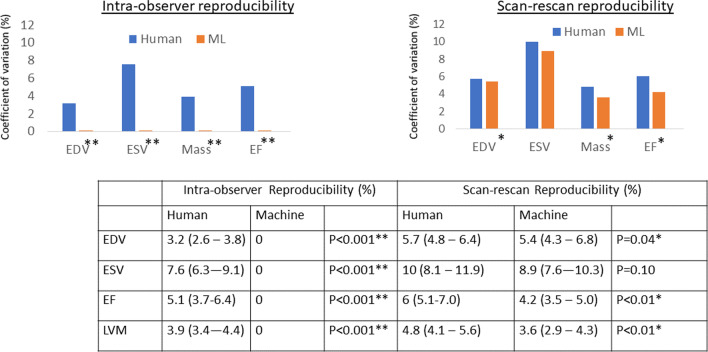
Findings: Machine analysis was quicker (20 s per patient) than human (13 min). Overall machine mis-segmentation rate was 1 in 479 images for the combined dataset, occurring mostly in rare pathologies not encountered in training. Without correcting these mis-segmentations, machine analysis had superior precision to three clinicians (e.g. scan-rescan coefficients of variation of human vs machine: LVEF 6.0% vs 4.2%, LV mass 4.8% vs. 3.6%; both P < 0.05), translating to a 46% reduction in required trial sample size using an LVEF endpoint.
Conclusion: We present a fully automated algorithm for measuring LV structure and global systolic function that betters human performance for speed and precision.
Keywords: Cardiac magnetic resonance; Cardiovascular imaging; Image processing; Machine learning; Ventricular function.
© 2022. The Author(s).
Conflict of interest statement
SEP reports personal fees from Circle Cardiovascular Imaging, outside of the submitted work.
Figures
References
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136:e137–e161. doi: 10.1161/CIR.0000000000000509. - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
-
- Dickstein K, Vardas PE, Auricchio A, et al. 2010 Focused Update of ESC Guidelines on device therapy in heart failure: an update of the 2008 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure and the 2007 ESC guidelines for cardiac and resynchronization therapy. Developed with the special contribution of the Heart Failure Association and the European Heart Rhythm Association. Eur Heart J. 2010;31:2677–2687. doi: 10.1093/eurheartj/ehq027. - DOI - PubMed
-
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:2768–2801. doi: 10.1093/eurheartj/ehw211. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
