

Evaluation of antithrombotic use and COVID-19 outcomes in a nationwide atrial fibrillation cohort
- PMID: 35273122
- PMCID: PMC8931797
- DOI: 10.1136/heartjnl-2021-320325
Evaluation of antithrombotic use and COVID-19 outcomes in a nationwide atrial fibrillation cohort
Abstract
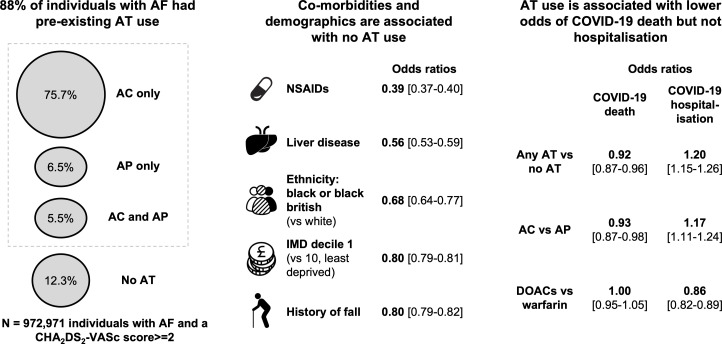
Objective: To evaluate antithrombotic (AT) use in individuals with atrial fibrillation (AF) and at high risk of stroke (CHA2DS2-VASc score ≥2) and investigate whether pre-existing AT use may improve COVID-19 outcomes.
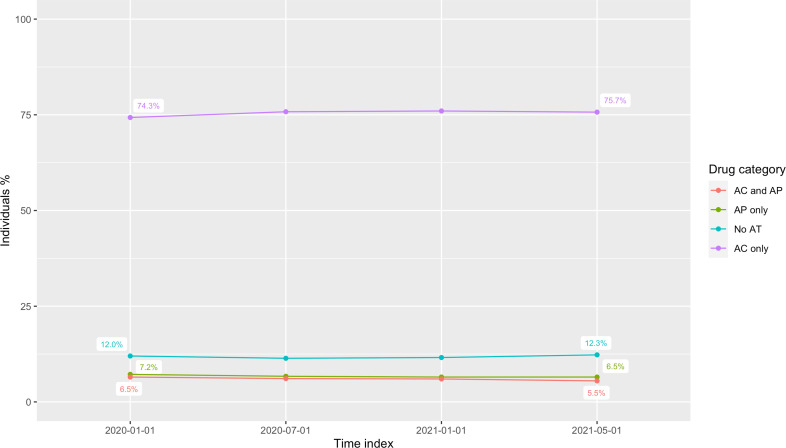
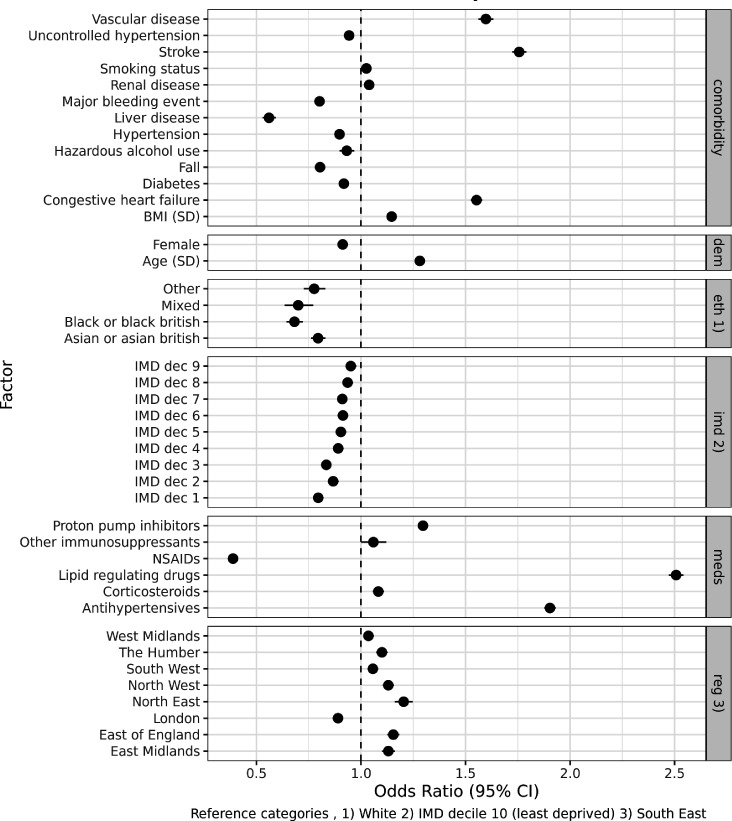
Methods: Individuals with AF and CHA2DS2-VASc score ≥2 on 1 January 2020 were identified using electronic health records for 56 million people in England and were followed up until 1 May 2021. Factors associated with pre-existing AT use were analysed using logistic regression. Differences in COVID-19-related hospitalisation and death were analysed using logistic and Cox regression in individuals with pre-existing AT use versus no AT use, anticoagulants (AC) versus antiplatelets (AP), and direct oral anticoagulants (DOACs) versus warfarin.
Results: From 972 971 individuals with AF (age 79 (±9.3), female 46.2%) and CHA2DS2-VASc score ≥2, 88.0% (n=856 336) had pre-existing AT use, 3.8% (n=37 418) had a COVID-19 hospitalisation and 2.2% (n=21 116) died, followed up to 1 May 2021. Factors associated with no AT use included comorbidities that may contraindicate AT use (liver disease and history of falls) and demographics (socioeconomic status and ethnicity). Pre-existing AT use was associated with lower odds of death (OR=0.92, 95% CI 0.87 to 0.96), but higher odds of hospitalisation (OR=1.20, 95% CI 1.15 to 1.26). AC versus AP was associated with lower odds of death (OR=0.93, 95% CI 0.87 to 0.98) and higher hospitalisation (OR=1.17, 95% CI 1.11 to 1.24). For DOACs versus warfarin, lower odds were observed for hospitalisation (OR=0.86, 95% CI 0.82 to 0.89) but not for death (OR=1.00, 95% CI 0.95 to 1.05).
Conclusions: Pre-existing AT use may be associated with lower odds of COVID-19 death and, while not evidence of causality, provides further incentive to improve AT coverage for eligible individuals with AF.
Keywords: COVID-19; atrial fibrillation; drug monitoring; electronic health records; epidemiology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Comment in
-
COVID-19: another reason for anticoagulation in patients with atrial fibrillation.Heart. 2022 May 25;108(12):902-904. doi: 10.1136/heartjnl-2022-320845. Heart. 2022. PMID: 35314451 No abstract available.
References
-
- NICE . Recommendations | atrial fibrillation: diagnosis and management | guidance | NICE, 2021. Available: https://www.nice.org.uk/guidance/ng196/chapter/Recommendations#stroke-pr... [Accessed 30 Jun 2021].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical