

Short-term inhalation of isoflurane improves the outcomes of intraportal hepatocyte transplantation
- PMID: 35273344
- PMCID: PMC8913608
- DOI: 10.1038/s41598-022-08237-6
Short-term inhalation of isoflurane improves the outcomes of intraportal hepatocyte transplantation
Abstract
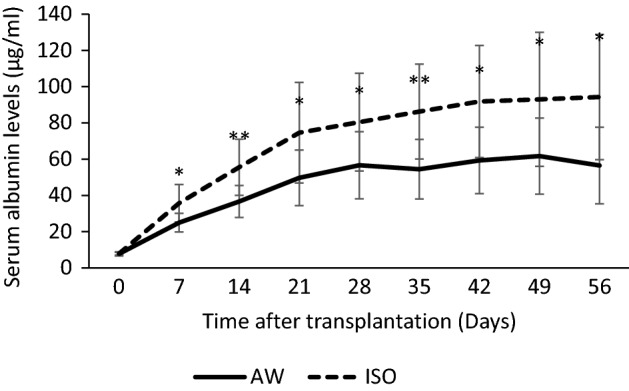
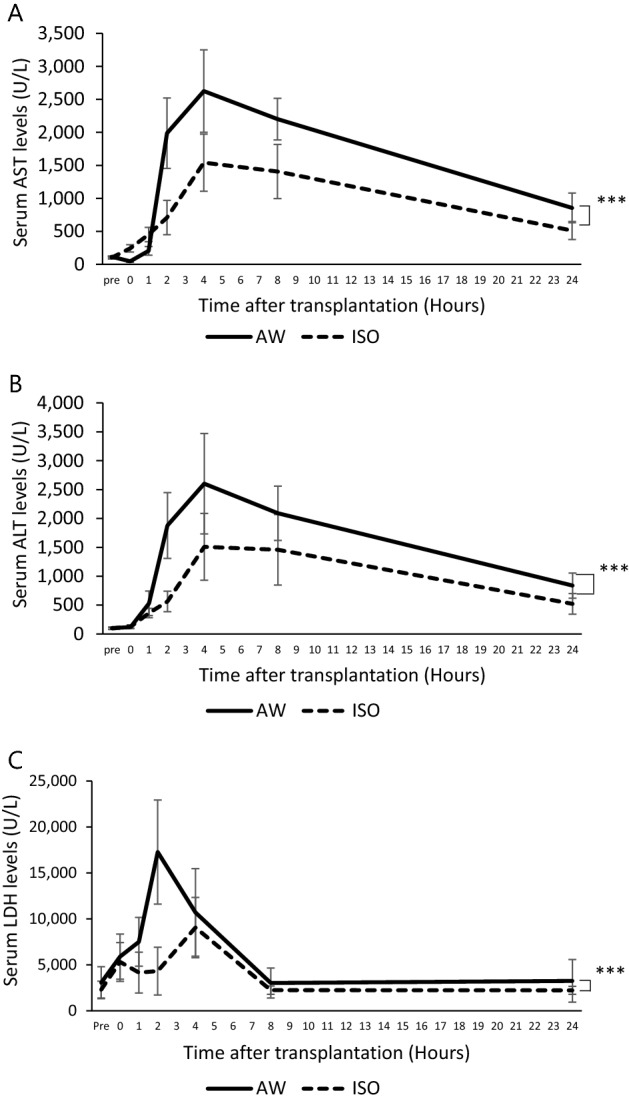
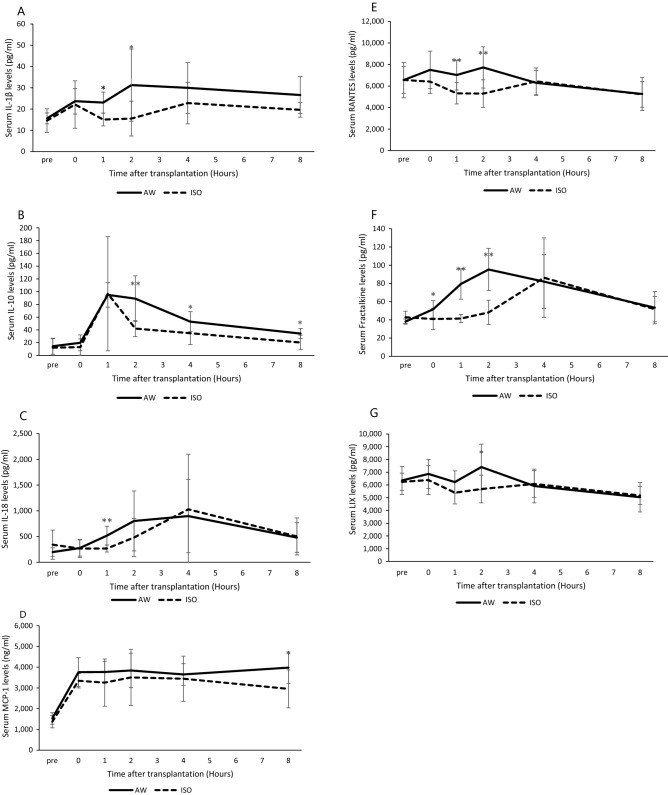
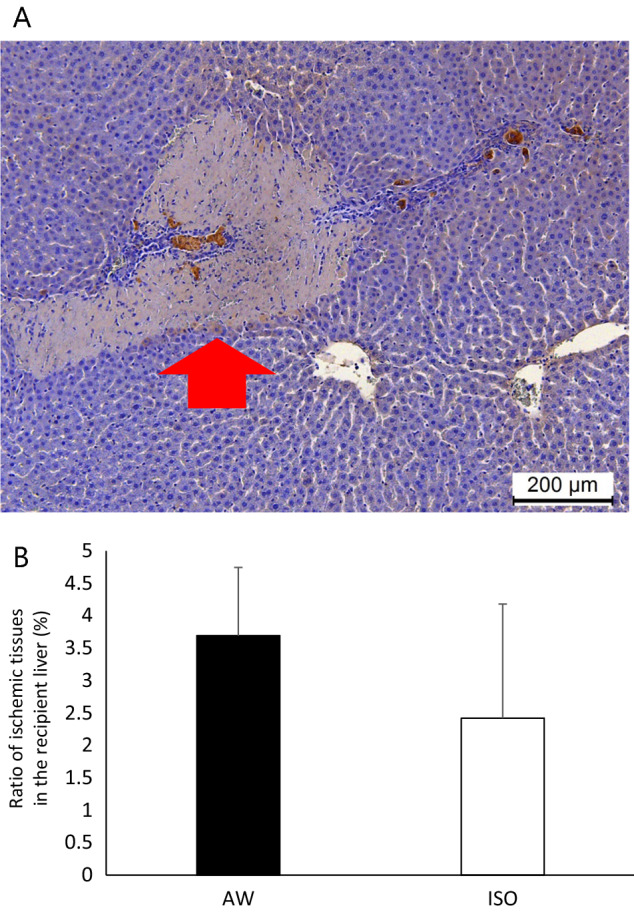
Clinical hepatocyte transplantation (HTx) is only performed without general anesthesia, while inhalation anesthetics are usually used in animal experiments. We hypothesized that isoflurane may be a possible reason for the discrepancy between the results of animal experiments and the clinical outcomes of HTx. Syngeneic rat hepatocytes (1.0 × 107) were transplanted to analbuminemic rats with (ISO group) and without (AW group) isoflurane. The serum albumin, AST, ALT, LDH levels and several inflammatory mediators were analyzed. Immunohistochemical staining and ex vivo imaging were also performed. The serum albumin levels of the ISO group were significantly higher in comparison to the AW group (p < 0.05). The serum AST, ALT, LDH levels of the ISO group were significantly suppressed in comparison to the AW group (p < 0.0001, respectively). The serum IL-1β, IL-10, IL-18, MCP-1, RNTES, Fractalkine and LIX levels were significantly suppressed in the ISO group. The ischemic regions of the recipient livers in the ISO group tended to be smaller than the AW group; however, the distribution of transplanted hepatocytes in the liver parenchyma was comparable between the two groups. Isoflurane may at least in part be a reason for the discrepancy between the results of animal experiments and the clinical outcomes of HTx.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Graziadei I, et al. Indications for liver transplantation in adults : Recommendations of the Austrian Society for Gastroenterology and Hepatology (ÖGGH) in cooperation with the Austrian Society for Transplantation, Transfusion and Genetics (ATX) Wien Klin. Wochenschr. 2016;128:679–690. doi: 10.1007/s00508-016-1046-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
