

Predictive factors, preventive implications, and personalized surgical strategies for bone metastasis from lung cancer: population-based approach with a comprehensive cancer center-based study
- PMID: 35273659
- PMCID: PMC8897531
- DOI: 10.1007/s13167-022-00270-9
Predictive factors, preventive implications, and personalized surgical strategies for bone metastasis from lung cancer: population-based approach with a comprehensive cancer center-based study
Abstract
Background: Bone metastasis (BM) and skeletal-related events (SREs) happen to advanced lung cancer (LC) patients without warning. LC-BM patients are often passive to BM diagnosis and surgical treatment. It is necessary to guide the diagnosis and treatment paradigm for LC-BM patients from reactive medicine toward predictive, preventive, and personalized medicine (PPPM) step by step.
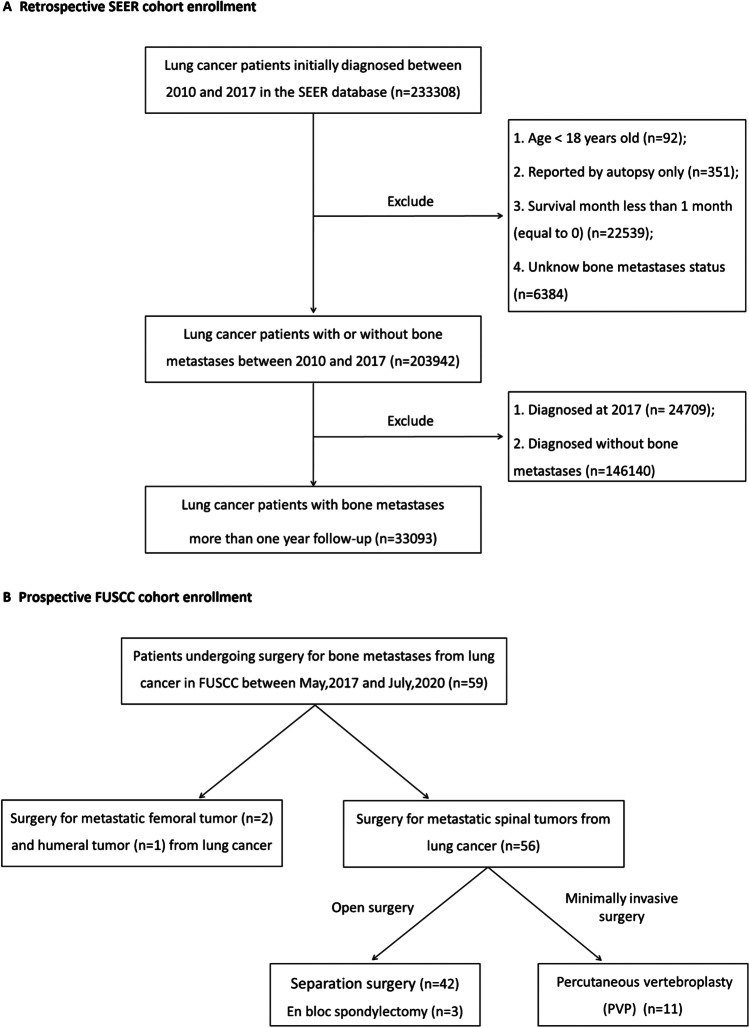
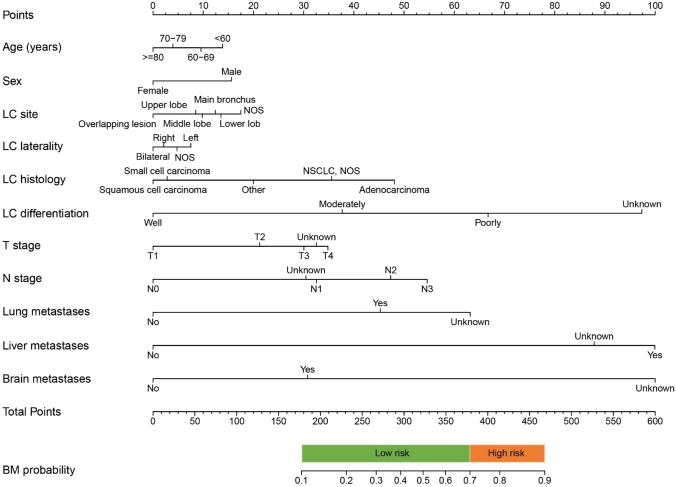
Methods: Two independent study cohorts including LC-BM patients were analyzed, including the Surveillance, Epidemiology, and End Results (SEER) cohort (n = 203942) and the prospective Fudan University Shanghai Cancer Center (FUSCC) cohort (n = 59). The epidemiological trends of BM in LC patients were depicted. Risk factors for BM were identified using a multivariable logistic regression model. An individualized nomogram was developed for BM risk stratification. Personalized surgical strategies and perioperative care were described for FUSCC cohort.
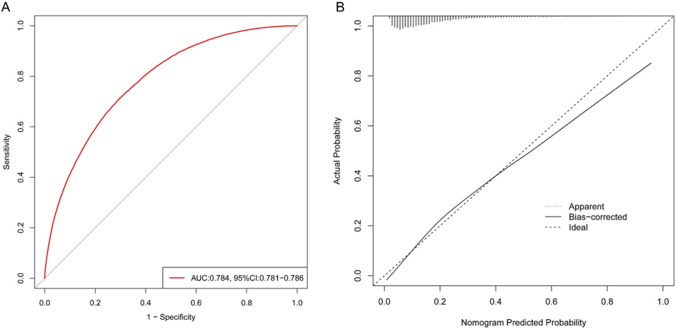
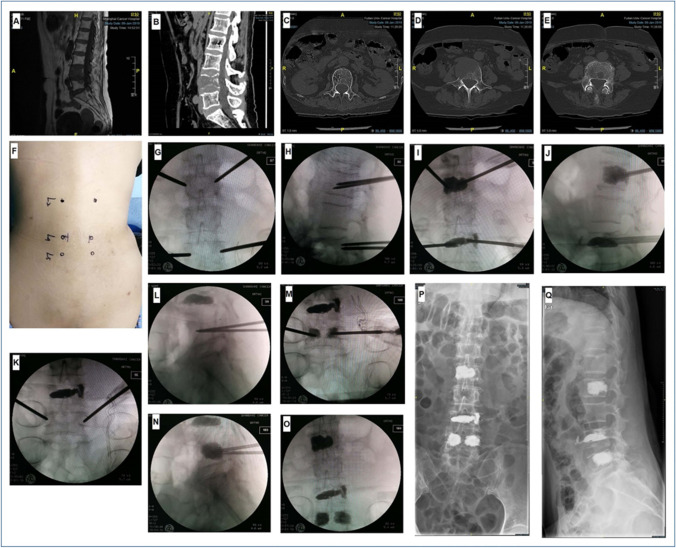
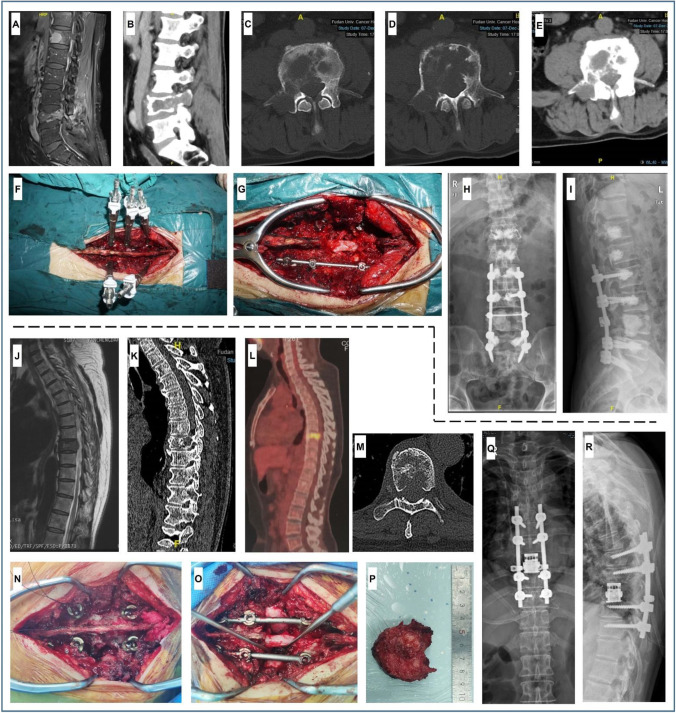
Results: The BM incidence rate in LC patients grew (from 17.53% in 2010 to 19.05% in 2016). Liver metastasis was a significant risk factor for BM (OR = 4.53, 95% CI = 4.38-4.69) and poor prognosis (HR = 1.29, 95% CI = 1.25-1.32). The individualized nomogram exhibited good predictive performance for BM risk stratification (AUC = 0.784, 95%CI = 0.781-0.786). Younger patients, males, patients with high invasive LC, and patients with other distant site metastases should be prioritized for BM prevention. Spine is the most common site of BM, causing back pain (91.5%), pathological vertebral fracture (27.1%), and difficult walking (25.4%). Spinal surgery with personalized spinal reconstruction significantly relieved pain and improved daily activities. Perioperative inflammation, immune, and nutrition abnormities warrant personalized managements. Radiotherapy needs to be recommended for specific postoperative individuals.
Conclusions: The presence of liver metastasis is a strong predictor of LC-BM. It is recommended to take proactive measures to prevent BM and its SREs, particularly in young patients, males, high invasive LC, and LC with liver metastasis. BM surgery and perioperative management are personalized and required. In addition, adjuvant radiation following separation surgery must also be included in PPPM-guided management.
Supplementary information: The online version contains supplementary material available at 10.1007/s13167-022-00270-9.
Keywords: Adjuvant radiation; Bone metastasis; Cancer; Lung cancer; Metastatic spinal tumors; Multidisciplinary team; Perioperative management; Personalization of medical services; Predictive factors; Predictive preventive personalized medicine (PPPM); Risk assessment; Surgery; Targeted prevention.
© The Author(s), under exclusive licence to European Association for Predictive, Preventive and Personalised Medicine (EPMA) 2022.
Conflict of interest statement
Conflict of interestThe authors declare no competing interests.
Figures


References
-
- Fornetti J, Welm AL, Stewart SA. Understanding the bone in cancer metastasis. J Bone Miner Res. 2018;33(12):2099–2113. - PubMed
-
- Choi SH, Koo JW, Choe D, et al. The incidence and management trends of metastatic spinal tumors in South Korea: a nationwide population-based study. Spine. 2020;45(14):E856–E863. - PubMed
-
- Adogwa O, Rubio DR, Buchowski JM, et al. Spine-specific skeletal related events and mortality in non-small cell lung cancer patients: a single-institution analysis. J Neurosurg Spine. 2020;27:1–8. - PubMed
-
- Shih JT, Yeh TT, Wang SH, et al. Incidence of bone metastases in patients with organ-specific cancers: a nationwide population-based cohort study. Int J Clin Pract. 2021;5:e13997. - PubMed
-
- Ryan C, Stoltzfus KC, Horn S, et al. Epidemiology of bone metastases. Bone. 2020;1:115783. - PubMed
LinkOut - more resources
Full Text Sources
