

Surgical Treatment of Spinal Fracture in a Patient With Ankylosing Spondylitis: An Opportunity To Correct Spinal Deformity Simultaneously With Fracture Fixation?
- PMID: 35273877
- PMCID: PMC8900830
- DOI: 10.7759/cureus.21936
Surgical Treatment of Spinal Fracture in a Patient With Ankylosing Spondylitis: An Opportunity To Correct Spinal Deformity Simultaneously With Fracture Fixation?
Abstract
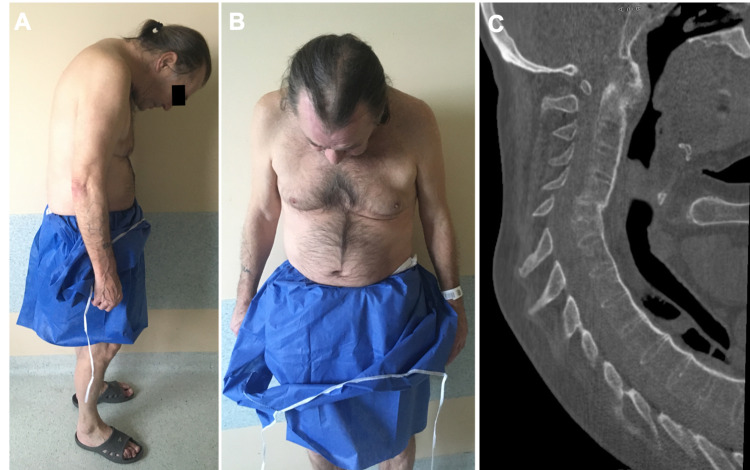
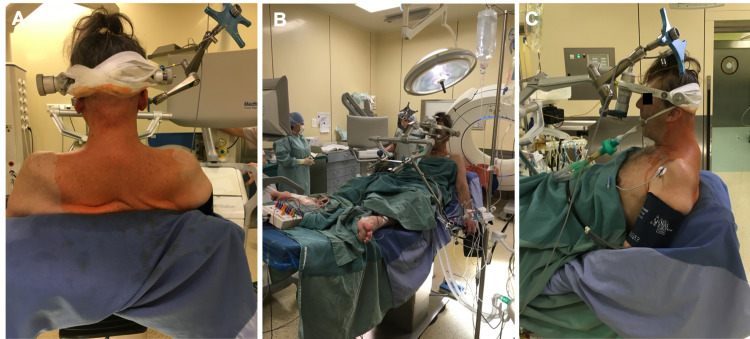
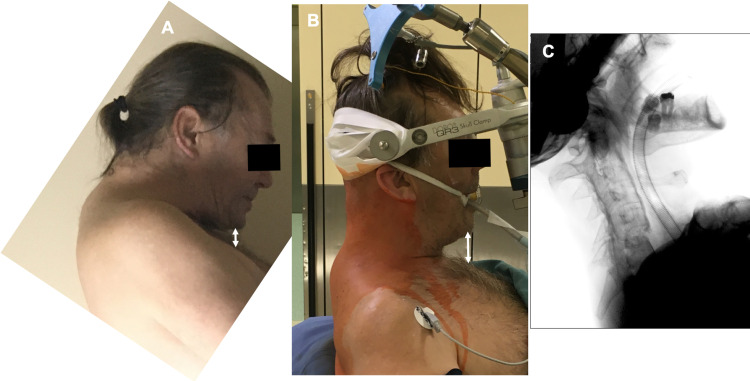
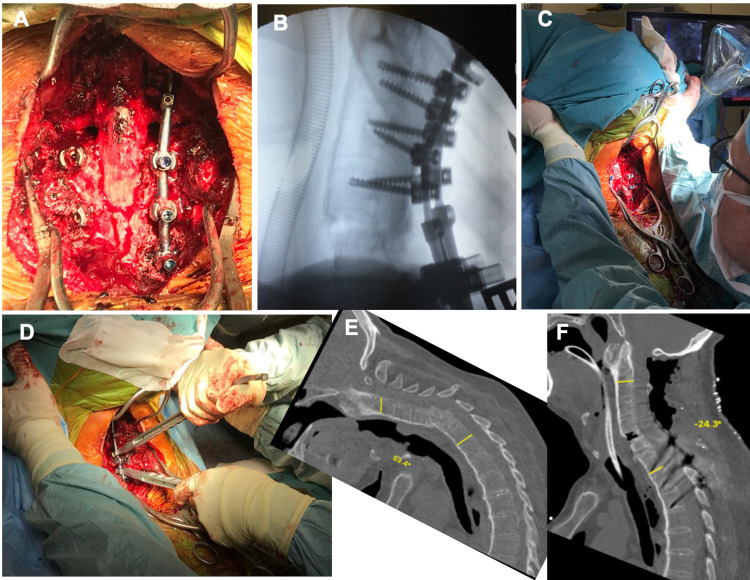
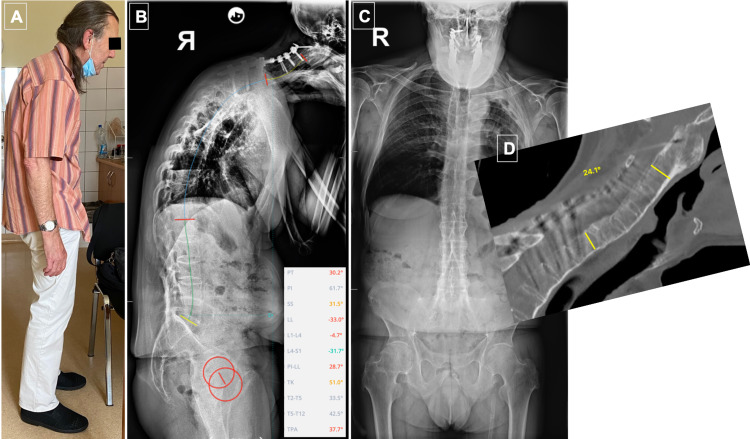
The objective of this case report is to describe the substantial sagittal correction of spinal hyperkyphosis alongside fracture fixation. In advanced ankylosing spondylitis (AS), the spine is usually fused, hyperkyphotic, and due to deformity, as well as improper bone remodeling, predisposed to fractures. These fractures, mostly unstable, require surgical treatment. The authors present fracture management with concomitant deformity correction at the fracture site and pedicle subtraction osteotomy (PSO) below the fracture, showing the benefits of performing the procedures with the patient in a sitting position. A 58-year-old male with AS was diagnosed with a fracture of C6 and referred to the department of neurosurgery, Wroclaw University Hospital. For the last week, he had complained of worsening neck pain and exacerbation of spinal kyphosis, with no neurological deficits. The patient had a fully fused spine, significant hyperkyphosis prior to the injury, and a fracture with an additionally exacerbated deformity. The patient was offered operative treatment - spinal fusion and fracture reduction with hyperkyphosis correction. The procedure consisted of 1) partial, mostly closed correction at the fracture site, 2) PSO of C7 and C2-T3 pedicular fixation and fusion while sitting in the posterior approach. To enable closed reduction at the fracture site and avoid difficulties with positioning a prone patient with very severe hyperkyphosis and an unstable spine, the authors performed surgical procedures with the patient in a sitting position. The authors obtained significant correction during the procedure by 740, from 53.40 of kyphosis to 24.30 of lordosis measured between C2 and T1. The patient had several complications (transient weakness of the upper limb, pleural effusion, and delayed wound healing); however, all resolved and the patient was discharged within two weeks post the operation. In patients with spinal hyperkyphosis with AS who sustain spinal fractures requiring operative treatment, it is worth considering simultaneous correction of the spinal deformity during surgical management of the fracture.
Keywords: ankylosing spondylitis; cervical fracture; hyperkyphosis; pedicle subtraction osteotomy; spinal surgery.
Copyright © 2022, Urbański et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Osteoporosis and vertebral fractures in ankylosing spondylitis. Davey-Ranasinghe N, Deodhar A. Curr Opin Rheumatol. 2013;25:509–516. - PubMed
-
- Spinal fractures in patients with ankylosing spondylitis. Leone A, Marino M, Dell'Atti C, Zecchi V, Magarelli N, Colosimo C. Rheumatol Int. 2016;36:1335–1346. - PubMed
-
- Spine fractures in patients with ankylosing spinal disorders. Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine (Phila Pa 1976) 2010;35:0–64. - PubMed
-
- Fractures in spinal ankylosing disorders: a narrative review of disease and injury types, treatment techniques, and outcomes. Rustagi T, Drazin D, Oner C, et al. J Orthop Trauma. 2017;31 Suppl 4:0–74. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous