

Supramaximal Horizontal Rectus Recession-Resection Surgery for Complete Unilateral Abducens Nerve Palsy
- PMID: 35273968
- PMCID: PMC8901715
- DOI: 10.3389/fmed.2021.795665
Supramaximal Horizontal Rectus Recession-Resection Surgery for Complete Unilateral Abducens Nerve Palsy
Abstract
Purpose: To review the surgical procedures and outcomes of supramaximal horizontal rectus recession-resection surgery for abduction deficiency and esotropia resulting from complete unilateral abducens nerve palsy.
Methods: A total of 36 consecutive cases diagnosed as complete abducens nerve palsy, receiving supramaximal medial rectus recession (8.5 ± 1.4 mm, range: 6-10) combined with a supramaximal lateral rectus resection (11.1 ± 1.7 mm, range: 8-14) as performed over the period from 2017 to 2020, were reviewed retrospectively. All surgeries were performed by a single surgeon. Pre- and post-operative ocular motility, ocular alignment, forced duction test, binocular vision, abnormal head posture, and surgical complications were assessed.
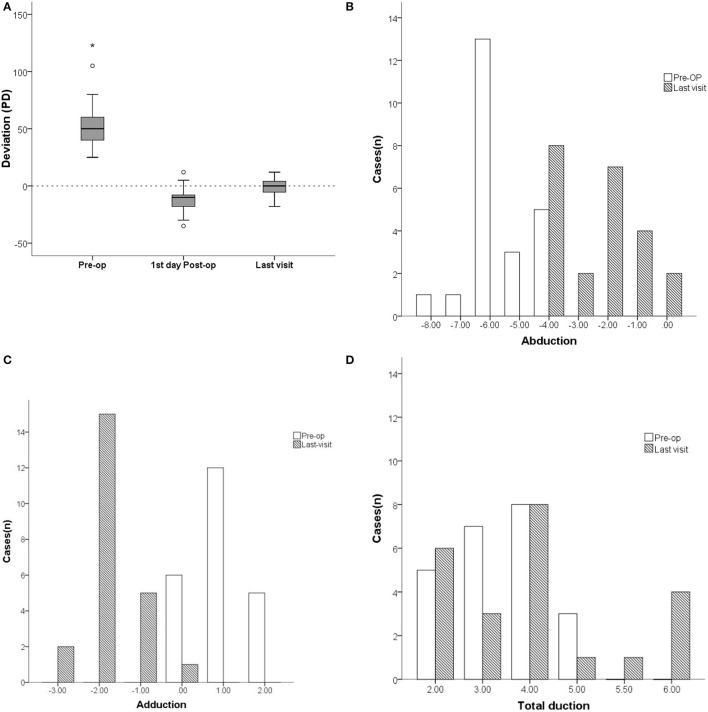
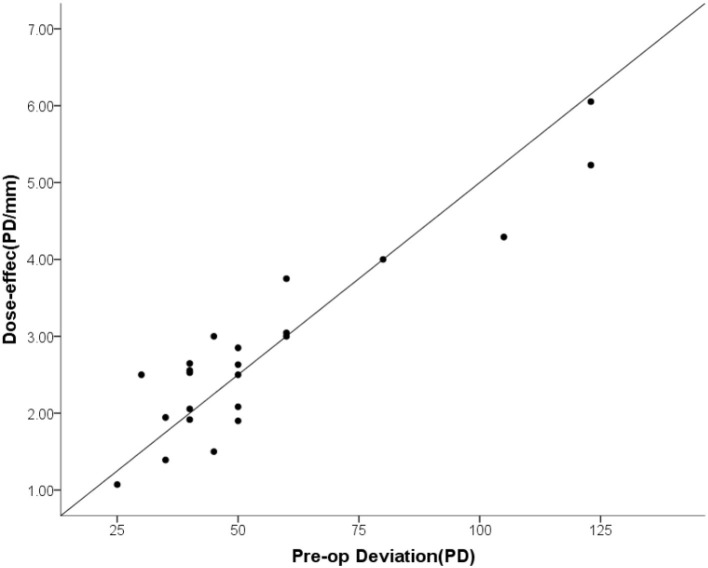
Results: Of these 36 cases, 23 (63.8%) were followed up for greater than 2 months (Mean ± SD = 8.4 ± 6.0, range: 2-24) after surgery and the collected data was presented. Mean ± SD age of these patients was 41.7 ± 14.4 (range: 12-67) years with 73.9% being female. Trauma (52.2%, 12/23) and cerebral lesions (21.7%, 5/23) were the primary etiologies for this condition. Esodeviation in primary position improved from 55.5 ± 27.2 prism diopters (PD) (range: +25 to +123) to 0.04 ± 7.3 PD (range: -18 to +12) as assessed on their last visit. Pre-operative abduction deficits of -5.6 ± 1.0 (range: -8 to -4) reduced to -2.4 ± 1.4 (range: -4 to 0) post-operatively. The mean dose-effect coefficient of 2.80 ± 1.20 PD/mm (range: 1.07-6.05) was positively correlated with pre-operative esodeviation. Rates of overcorrection and ortho were 69.6 and 26.1%, respectively, on the first day after surgery, while on their last visit the respective levels were 4.3 and 82.6%.
Conclusion: Supramaximal horizontal rectus recession-resection surgery is an effective treatment method for complete abduction deficiency. The dose-effect was positively correlated with pre-operative esodeviation. Overcorrection on the first day post-operatively is required for a long-term satisfactory surgical outcome.
Keywords: complete abducens palsy; paralytic strabismus; rectus recession-resection; surgical dosage-effect; surgical outcome.
Copyright © 2022 Wang, Fu, Shen, Qiu, Yu, Shen and Yan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Louis CV. Binocular Vision Ocular Motility. (2002), 446–8.
LinkOut - more resources
Full Text Sources