

Audit of long-term treatment outcomes of thyrotoxicosis in a single-centre virtual clinic: The utility of long-term antithyroid drugs
- PMID: 35274339
- PMCID: PMC9790704
- DOI: 10.1111/cen.14721
Audit of long-term treatment outcomes of thyrotoxicosis in a single-centre virtual clinic: The utility of long-term antithyroid drugs
Abstract
Objective: To investigate the long-term outcomes and prognosis of thyrotoxicosis in a large number of patients in a single UK county (Leicestershire).
Design: Retrospective cohort analysis of 56,741 thyroid function test (TFT) results, treatment modalities and outcomes in a well-established virtual thyrotoxicosis clinic database.
Patients: One thousand four hundred and eighty-nine patients were included with a median length of follow-up of 10.9 years. The aetiology of thyrotoxicosis was autoimmune (85.9%), nodular (9.1%) and mixed (5.0%). Treatment modalities included antithyroid drugs (ATDs), radioiodine (RAI; 555 MBq fixed dose) and thyroidectomy.
Methods: We analysed both individual TFTs and groups of sequential TFTs on or after the same thyroid treatment(s), which we describe as 'phase of thyroid care' (POTC). Patients studied entered the virtual clinic between 1 January 1995 and 1 January 2010; we exported data on every TFT sample up to April 2020.
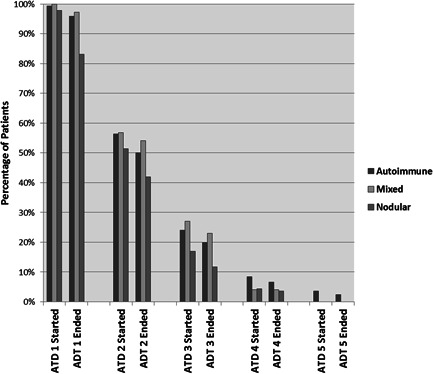
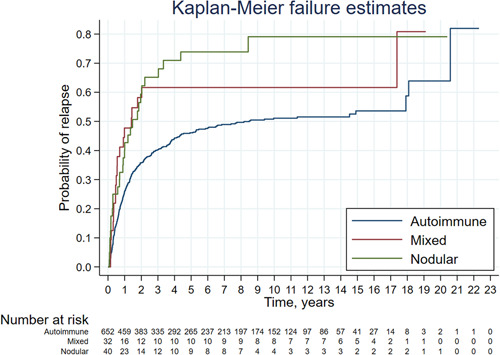
Results: ATD had been used in 99.2% (median 2, maximum seven courses) with long-term ATD (>2 years) in 48%. RAI and thyroidectomy were used more commonly with nodular and mixed aetiology. Overall, T4 was more often controlled than thyroid-stimulating hormone (TSH), and at the latest follow-up, T4 was normal in >96%, TSH in >79% and both in >76% of different aetiologies. The mean percentage control of T4 was 85% and TSH 50%; in long-term ATD courses, this improved to 89% and 62%, respectively. In the latest POTC, control of T4 and TSH was best in cases off treatment (95%/87%) and on T4 without ablative therapy (94%/72%), but was broadly similar in patients on long-term ATD (90%/68%), after RAI (92%/60%) or after thyroidectomy (91%/58%). After the first course of ATD, remission or hypothyroidism was seen in 47.3% autoimmune, 20.9% nodular and 32.5% mixed, with 90% relapses seen within 4 years. Relapse was more common in patients with ophthalmopathy, but there was no difference between the sexes.
Conclusions: Thyrotoxicosis can be well controlled with minimal specialist clinic attendance using a software-supported virtual shared-care scheme. Long-term ATD appears to be a valid patient choice achieving TFT control comparable to that seen after RAI or surgery. In patients with autoimmune disease, relapse is more common in patients with ophthalmopathy, and hypothyroidism is common after RAI. In nodular disease, we found that spontaneous remission may occur.
Keywords: carbimazole; hyperthyroidism; radioiodine; thyroid; thyrotoxicosis; virtual clinic.
© 2022 The Authors. Clinical Endocrinology published by John Wiley & Sons Ltd.
Figures
References
-
- NICE National Institute for Health and Care Excellence .Thyroid Disease: Assessment and Management. NICE Guideline (NG145). 2019. - PubMed
-
- Ross DS, Burch HB, Cooper DS, et al. American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343‐1421. - PubMed
-
- Codaccioni JL, Orgiazzi J, Blanc P, Pugeat M, Roulier R, Carayon P. Lasting remissions in patients treated for Graves' hyperthyroidism with propranolol alone: a pattern of spontaneous evolution of the disease. J Clin Endocrinol Metab. 1988;67(4):656‐662. - PubMed
-
- Wartofsky L, Glinoer D, Solomon B, et al. Differences and similarities in the diagnosis and treatment of Graves' disease in Europe, Japan, and the United States. Thyroid. 1991;1:129‐135. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
