

Triple therapy with artemether-lumefantrine plus amodiaquine versus artemether-lumefantrine alone for artemisinin-resistant, uncomplicated falciparum malaria: an open-label, randomised, multicentre trial
- PMID: 35276064
- PMCID: PMC9132777
- DOI: 10.1016/S1473-3099(21)00692-7
Triple therapy with artemether-lumefantrine plus amodiaquine versus artemether-lumefantrine alone for artemisinin-resistant, uncomplicated falciparum malaria: an open-label, randomised, multicentre trial
Erratum in
-
Correction to Lancet Infect Dis 2022; published online March 8. https://doi.org/10.1016/S1473-3099(21)00692-7.Lancet Infect Dis. 2022 May;22(5):e128. doi: 10.1016/S1473-3099(22)00220-1. Epub 2022 Mar 28. Lancet Infect Dis. 2022. PMID: 35358428 Free PMC article. No abstract available.
Abstract
Background: Late treatment failures after artemisinin-based combination therapies (ACTs) for falciparum malaria have increased in the Greater Mekong subregion in southeast Asia. Addition of amodiaquine to artemether-lumefantrine could provide an efficacious treatment for multidrug-resistant infections.
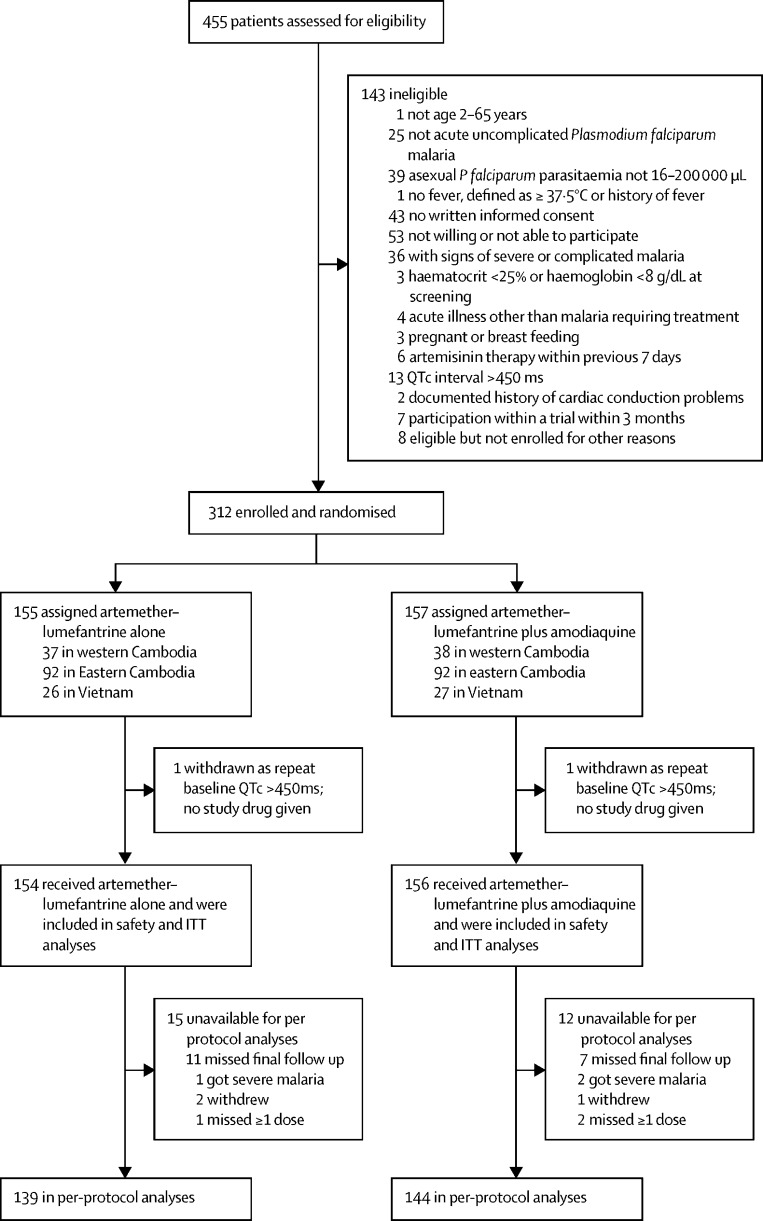
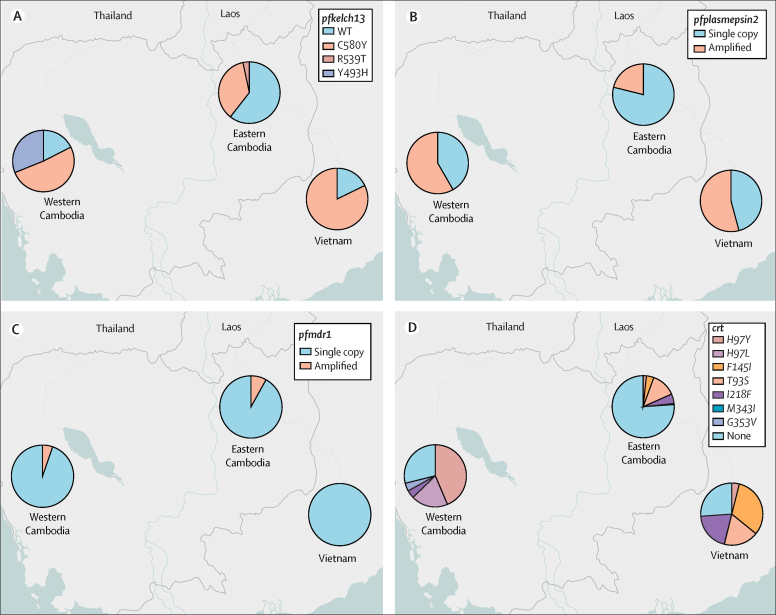
Methods: We conducted an open-label, randomised trial at five hospitals or health centres in three locations (western Cambodia, eastern Cambodia, and Vietnam). Eligible participants were male and female patients aged 2-65 years with uncomplicated Plasmodium falciparum malaria. Patients were randomly allocated (1:1 in blocks of eight to 12) to either artemether-lumefantrine alone (dosed according to WHO guidelines) or artemether-lumefantrine plus amodiaquine (10 mg base per kg/day), both given orally as six doses over 3 days. All received a single dose of primaquine (0·25 mg/kg) 24 h after the start of study treatment to limit transmission of the parasite. Parasites were genotyped, identifying artemisinin resistance. The primary outcome was Kaplan-Meier 42-day PCR-corrected efficacy against recrudescence of the original parasite, assessed by intent-to-treat. Safety was a secondary outcome. This completed trial is registered at ClinicalTrials.gov (NCT03355664).
Findings: Between March 18, 2018, and Jan 30, 2020, 310 patients received randomly allocated treatment; 154 received artemether-lumefantrine alone and 156 received artemether-lumefantrine plus amodiaquine. Parasites from 305 of these patients were genotyped. 42-day PCR-corrected treatment efficacy was noted in 151 (97%, 95% CI 92-99) of 156 patients with artemether-lumefantrine plus amodiaquine versus 146 (95%, 89-97) of 154 patients with artemether-lumefantrine alone; hazard ratio (HR) for recrudescence 0·6 (95% CI 0·2-1·9, p=0·38). Of the 13 recrudescences, 12 were in 174 (57%) of 305 infections with pfkelch13 mutations indicating artemisinin resistance, for which 42-day efficacy was noted in 89 (96%) of 93 infections with artemether-lumefantrine plus amodiaquine versus 73 (90%) of 81 infections with artemether-lumefantrine alone; HR for recrudescence 0·44 (95% CI 0·14-1·40, p=0·17). Artemether-lumefantrine plus amodiaquine was generally well tolerated, but the number of mild (grade 1-2) adverse events, mainly gastrointestinal, was greater in this group compared with artemether-lumefantrine alone (vomiting, 12 [8%] with artemether-lumefantrine plus amodiaquine vs three [2%] with artemether-lumefantrine alone, p=0·03; and nausea, 11 [7%] with artemether-lumefantrine plus amodiaquine vs three [2%] with artemether-lumefantrine alone, p=0·05). Early vomiting within 1 h of treatment, requiring retreatment, occurred in no patients of 154 with artemether-lumefantrine alone versus five (3%) of 156 with artemether-lumefantrine plus amodiaquine, p=0·06. Bradycardia (≤54 beats/min) of any grade was noted in 59 (38%) of 154 patients with artemether-lumefantrine alone and 95 (61%) of 156 with artemether-lumefantrine plus amodiaquine, p=0·0001.
Interpretation: Artemether-lumefantrine plus amodiaquine provides an alternative to artemether-lumefantrine alone as first-line treatment for multidrug-resistant P falciparum malaria in the Greater Mekong subregion, and could prolong the therapeutic lifetime of artemether-lumefantrine in malaria-endemic populations.
Funding: Bill & Melinda Gates Foundation, Wellcome Trust.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests The Mahidol Oxford Research Unit (MORU) has received funding for other studies of antimalarial treatment from Fosun Pharmaceuticals, which manufactures artemisinin combination therapies. We declare no other competing interests.
Figures

Comment in
-
Triple artemisinin-based combination therapies for malaria: a timely solution to counter antimalarial drug resistance.Lancet Infect Dis. 2022 Jun;22(6):751-753. doi: 10.1016/S1473-3099(21)00748-9. Epub 2022 Mar 8. Lancet Infect Dis. 2022. PMID: 35276063 No abstract available.
-
Is triple artemisinin-based combination therapy necessary for uncomplicated malaria?Lancet Infect Dis. 2022 May;22(5):586-587. doi: 10.1016/S1473-3099(22)00209-2. Lancet Infect Dis. 2022. PMID: 35460650 No abstract available.
-
Is triple artemisinin-based combination therapy necessary for uncomplicated malaria?Lancet Infect Dis. 2022 Jun;22(6):765-766. doi: 10.1016/S1473-3099(22)00283-3. Lancet Infect Dis. 2022. PMID: 35643100 Free PMC article. No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2015. Strategy for malaria elimination in the Greater Mekong subregion (2015–2030)
-
- Medicines for Malaria Venture Product availability maps. 2021. https://www.mmv.org/access/product-maps
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
