

Development and validation of a gradient boosting machine to predict prognosis after liver resection for intrahepatic cholangiocarcinoma
- PMID: 35277130
- PMCID: PMC8915487
- DOI: 10.1186/s12885-022-09352-3
Development and validation of a gradient boosting machine to predict prognosis after liver resection for intrahepatic cholangiocarcinoma
Abstract
Background: Accurate prognosis assessment is essential for surgically resected intrahepatic cholangiocarcinoma (ICC) while published prognostic tools are limited by modest performance. We therefore aimed to establish a novel model to predict survival in resected ICC based on readily-available clinical parameters using machine learning technique.
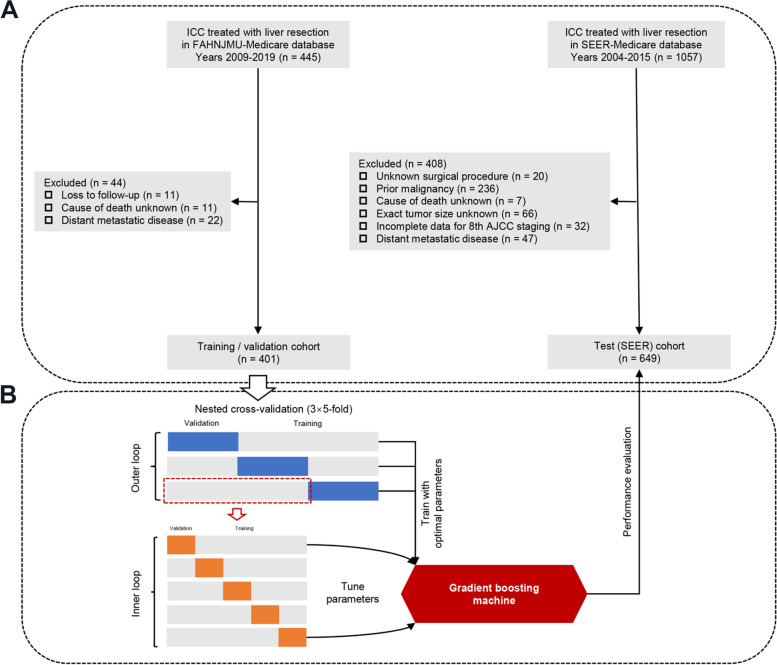
Methods: A gradient boosting machine (GBM) was trained and validated to predict the likelihood of cancer-specific survival (CSS) on data from a Chinese hospital-based database using nested cross-validation, and then tested on the Surveillance, Epidemiology, and End Results (SEER) database. The performance of GBM model was compared with that of proposed prognostic score and staging system.
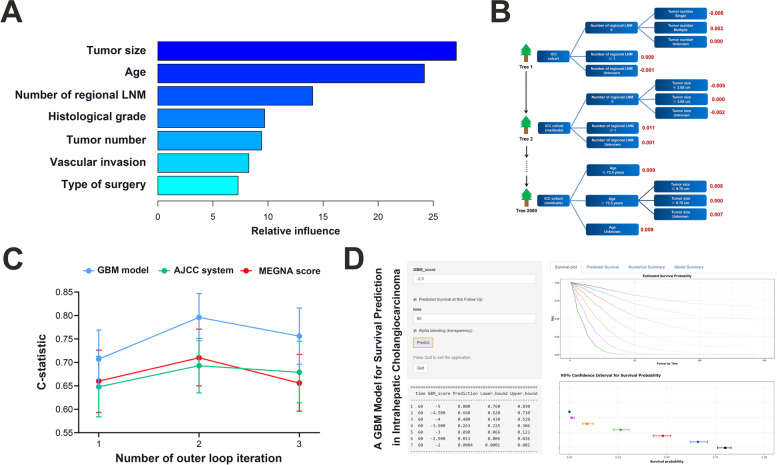
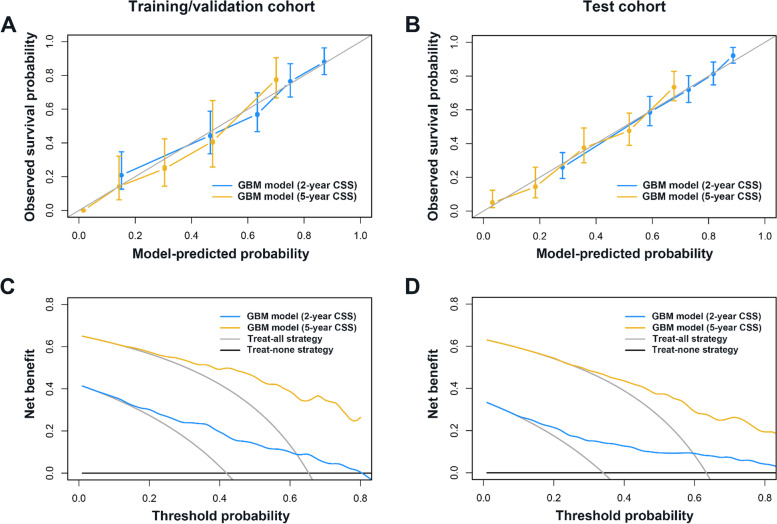
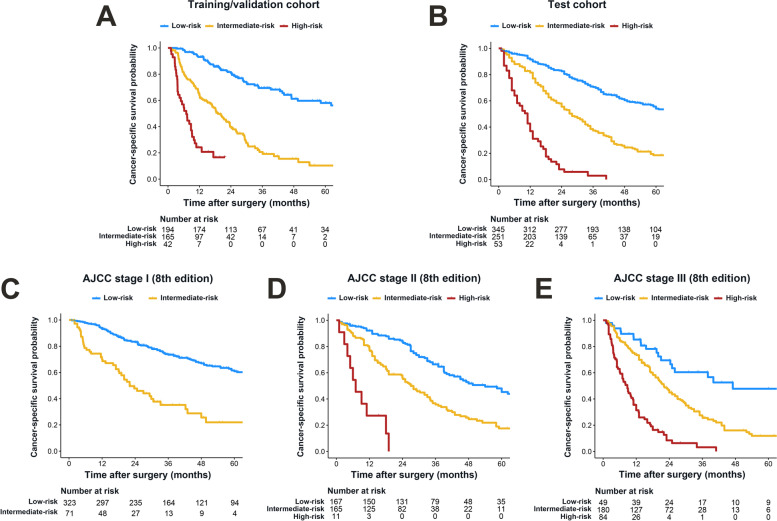
Results: A total of 1050 ICC patients (401 from China and 649 from SEER) treated with resection were included. Seven covariates were identified and entered into the GBM model: age, tumor size, tumor number, vascular invasion, number of regional lymph node metastasis, histological grade, and type of surgery. The GBM model predicted CSS with C-Statistics ≥ 0.72 and outperformed proposed prognostic score or system across study cohorts, even in sub-cohort with missing data. Calibration plots of predicted probabilities against observed survival rates indicated excellent concordance. Decision curve analysis demonstrated that the model had high clinical utility. The GBM model was able to stratify 5-year CSS ranging from over 54% in low-risk subset to 0% in high-risk subset.
Conclusions: We trained and validated a GBM model that allows a more accurate estimation of patient survival after resection compared with other prognostic indices. Such a model is readily integrated into a decision-support electronic health record system, and may improve therapeutic strategies for patients with resected ICC.
Keywords: Intrahepatic cholangiocarcinoma; Machine learning; Modelling; Surgery; Survival.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
